

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
A number of recent clinical studies have reported marked target organ damages in patients with primary aldosteronism. The aim of this study was to compare the incidence of target organ damages in patients with primary aldosteronism (PA) and essential hypertension (EHT).
Methods
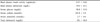
The clinical records of 41 PA patients, over a 20-year period, were retrospectively analyzed. The clinical characteristics and incidence of target organ damages of 33 of the patients in this group were compared with those of 66 patients with essential hypertension, directly matched for age, gender and mean blood pressure. 8 of the PA patients could not be matched with EHT patients for age, gender and mean blood pressure, so were excluded from the comparison. The patients with essential hypertension were sampled from patients who visited for the evaluation of hypertension.
Results
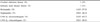
Ischemic heart diseases were found in 18.2 and 10.6% of patients with PA and EHT, respectively (P = 0.22). From echocardiograms, left ventricular hypertrophy was found in 93.3% and 61.4% of patients with PA and EHT, respectively (P = 0.017). The degrees of left ventricular hypertrophy were correlated with the levels of serum aldosterone, with an r value of 0.490 (P < 0.005). Cerebrovascular attack was found in 18.2% and 1.5% of patients with PA and EHT, respectively (P = 0.005). Hypertensive retinopathy was found in 50% and 33.3% of patients with PA and EHT (P = 0.255), and nephropathy was found in 42.4% and 25.8% of patients with PA and EHT, respectively (P = 0.074).
Figures and Tables





References
1. Young WF Jr. Minireview: primary aldosteronism-changing concepts in diagnosis and treatment. Endocrinology. 2003. 144:2208–2213.
2. Calhoun DA, Nishizaka MK, Zaman MA, Thakkar RB, Weissmann P. Hyperaldosteronism among black and white subjects with resistant hypertension. Hypertension. 2002. 40:892–896.
3. Dluhy RG, Williams GH. Aldosterone villain or bystander? N Eng J Med. 2004. 351:8–10.
4. Matsumura K, Fujii K, Oniki H, Oka M, Iida M. Role of aldosterone in left ventricular hypertrophy in hypertension. Am J Hypertens. 2006. 19:13–18.
5. Devereux RB, Reichek N. Determination of left ventricular mass in man: anatomic validation of the method. Circulation. 1977. 55:613–618.
6. Kwon SH, Cho YM, Park HK, Park DJ, Shin CS, Park KS, Kim SY, Cho BY, Lee HK. Hypertensive Complications in Patients with Primary Aldosteronism. J Kor Soc Endocrinol. 2002. 17:95–103.
7. Conn JW. Presidential address. Part I, Painting background. Part II, Primary aldosteronism, a new clinical syndrome. J Lab Clin Med. 1955. 45:3.
8. Brown CA, Bouldin MJ, Blackston JW, Duddleston DN, Shepherd JM, Hicks GS. Hyperaldosteronism: the internist's hypertensive disease. Am J Med Sci. 2002. 324:227–231.
9. Young WF Jr. Pheochromocytoma and primary aldosteronism: diagnostic approaches. Endocrinol Metab Clin North Am. 1997. 26:801–827.
10. Mulatero P, Stowasser M, Loh K-C, Fardella CE, Gordon R, Mosso L, Gomez-Sanchez CE, Veglio F, Young WF Jr. Extensive personal experience: Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab. 2004. 89:1045 –1050.
11. Magill SB, Raff H, Shaker JL, Brickner RC, Knechtges TE, Kehoe ME, Findling JW. Comparison of adrenal vein sampling and computed tomography in differentiation of primary aldosteronism. J Clin Endocrinol Metab. 2001. 86:1066–1071.
12. Lumachi F, Ermani M, Basso SM, Armanini D, Iacobone M, Favia G. Long-term results of adrenalectomy in patients with aldosterone-producing adenomas: multivariate analysis of factors affecting unresolved hypertension and review of the literature. Am Surg. 2005. 71:864–869.
13. Milliez P, Girerd X, Plouin PF, Blacher J, Safar ME, Mourad JJ. Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol. 2005. 45:1243–1248.
14. Takeda R, Matsubara T, Miyamori I, Hatakeyama H. Vascular complications in Patients with aldosterone producing adenoma in Japan: comparative study with essential hypertension. The Research Committee of Disorders of Adrenal Hormones in Japan. J Endocrinol Invest. 1995. 18:370–373.
15. Rossi GP, Cesari M, Sacchetto A. LVH in primary aldosteronism. Hypertension. 1997. 30:1297–1298.
16. Rossi GP, Sacchetto A, Pavan E, Palatini P, Graniero GR, Canali C, Pessina AC. Remodeling of the left ventricle in primary aldosteronism due to Conn's adenoma. Circulation. 1997. 95:1471–1478.
17. Dorrance AM, Osborn HL, Grekin R, Webb RC. Spironolactone reduces cerebral infarct size and EGF-receptor mRNA in stroke-prone rats. Am J Physiol Regul Integr Comp Physiol. 2001. 281:R944–R950.
18. MacLeod AB, Vasdev S, Smeda JS. The role of blood pressure and aldosterone in the production of hemorrhagic stroke in captopril-treated hypertensive rats. Stroke. 1997. 28:1821–1828.
19. Nishimura M, Uzu T, Fujii T, Kuroda S, Nakamura S, Inenaga T, Kimura G. Cardiovascular complications in patients with primary aldosteronism. Am J Kidney Dis. 1999. 33:261–266.
20. Fallo F, Veglio F, Bertello C, Sonino N, Della Mea P, Ermani M, Rabbia F, Federspil G, Mulatero P. Prevalence and characteristics of the metabolic syndrome in primary aldosteronism. J Clin Endocrinol Metab. 2006. 91:454–459.
 XML Download
XML Download