

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Incidentaloma is defined as an asymptomatic mass lesion that shows no associated hormonal hyper- or hyposecretion. Adrenal incidentaloma is also a typical mass detection of which is known to have increased with improved imaging techniques such as CT or MRI. We report a case in which a pituitary incidentaloma is accompanied by an adrenal incidentaloma. The 65-year-old patient was admitted due to oropharyngeal pain, and had a medical history that included an operation for rectal cancer. The adrenal tumor had no function, but left adrenalectomy was performed for the evaluation of rectal cancer recurrence, which was diagnosed pathologically as a benign adrenocortical nodule. In our experience we have found that, in the case of multiple incidentalomas, it is important to evaluate the function or malignancy status of each.
Figures and Tables
Fig. 1
Sellar MRI findings. It is shown as pituitary incidentaloma, such as macroadenoma. Right side erosion of floor of sella with surrounding slightly low and high signal intensity lesion extending into left side parasella with suprasella and relatively contrast enhancement with right side deviation of infundibulum, about 1.2 cm in length are noted.
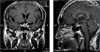
Fig. 2
Abdomen and pelvis CT findings. It is shown that nodular mass lesion on left adrenal area about 2.0 cm sized with homogenous and smooth margined wall which is like adrenal incidentaloma, but cannot be ruled out metastasis.



References
1. Mirilas P, Skandalakis JE. Benign anatomical mistakes: incidentaloma. Am Surg. 2002. 68:1026–1028.
2. Hall WA, Luciano MG, Doppman JL, Patronas NJ, Oldfield EH. Pituitary magnetic resonance imaging in normal human volunteers: occult adenomas in the general population. Ann Int Med. 1994. 120:817–820.
3. Peppercorn PD, Grossman AB, Reznek RH. Imaging of incidentally discovered adrenal masses. Clin Endocrinol (Oxf). 1998. 48:379–388.
4. Burgess JR, Greenaway TM, Shepherd JJ. Expression of the MEN-1 gene in a large kindred with multiple endocrine neoplasia type 1. J Intern Med. 1998. 243:465–470.
5. De Marinis L, Mancini A, Fiumara C, Conte G, La Brocca A, Sammartano L, Valle D, Danza F. A case of adrenal adenoma with radiologic "cystic" appearance associated with hypophyseal adenoma. Minerva Chir. 1993. 48:1331–1336.
6. Marchesa P, Fazio VW, Church JM, McGannon E. adrenal masses in patients with familial adenomatous polyposis. Dis Colon Rectum. 1997. 40:1023–1028.
7. Gross MD, Shapiro B. Clinical review 50: clinically silent adrenal masses. J Clin Endocrinol Metab. 1993. 77:885–888.
8. Barzon L, Boscaro M. Diagnosis and management of adrenal incidentaloma. J Urol. 2000. 163:398–407.
9. Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM. Incidentally discovered adrenal tumors: an institutional perspective. Surgery. 1991. 110:1014–1021.
10. Mantero F, Arnaldi G. Management approaches to adrenal incidentalomas: a view from Ancora, Italy. Endocrinol Metab Clin North Am. 2000. 29:107–125.
11. Bitter DA, Ross DS. Incidentally discovered adrenal masses. Am J Surg. 1989. 158:159–161.
12. Mantero F, Masini AM, Opocher G, Giobagnetti M, Arnaldi G. Adrenal incidentaloma: an overview of hormonal data from the National Italian Study Group. Horm Res. 1997. 47:284–289.
13. Jacobs JK, Goldstein RE, Geer RJ. Laparoscopic adrenalectomy. A new standard of care. Ann Surg. 1997. 225:495–501.
14. Silverman SG, Mueller PR, Pinkney LP, Koenker RM, Seltzer SE. Predictive value of image-guided adrenal biopsy: analysis and results of 101 biopsies. Radiology. 1993. 187:715–718.
15. Wolpert SM, Molitch ME, Goldman JA, Wood JB. Size, shape and appearance of the normal female pituitary gland. Am J Roentgenol. 1984. 143:377–381.
16. McComb DJ, Ryan N, Horvath E, Kovacs K. Subclinical adenomas of the human pituitary. New light on old problems. Arch Pathol Lab Med. 1983. 107:488–491.
17. Reincke M, Allolio B, Saeger W, Menzel J, Winkelmann W. The 'incidentaloma' of the pituitary gland. Is neurosurgery required? JAMA. 1990. 263:2772–2776.
 XML Download
XML Download