

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
An empty sella is defined as a sella which, regardless of its size, is completely or partly filled with cerebrospinal fluid. The endocrine function of primary empty sella syndrome is usually normal, but sometimes this syndrome is associated with complete or partial pituitary insufficiency and rarely hypersecretion of pituitary hormone. Primary empty sella syndrome combined with Cushing's disease has rarely been reported. A 45-years-old woman presented with cushingoid feature. Her urinary cortisol and 17-hydroxycorticosteroid excretion were increased. The results of endocrine function testing were suggestive of Cushing's disease. Sella MRI showed of partially empty sella and pituitary microadenoma. The pituitary microadenoma was removed by the trans-sphenoidal approach. We report here on this case together with a review of the literature.
Figures and Tables
Fig. 1
MRI of pituitary gland. A. Coronal T1-weighted MR scan shows a partially empty sella; B. Coronal post contrast T1-weighted MR scan shows a tiny hypointense lesion within the enhancing pituitary gland (5 × 4.9 mm in size).
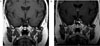
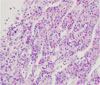
Fig. 2
Histology of the resected pituitary mass. Microscopic appearance of (H&E stain, × 100) panel shows solid sheet of neoplastic cells with intervening vascular channels. The indivisual cell are round to oval nucleus with acidophilic and clear cytoplasm.


References
1. Busch W. Die morphologie der sella turcica und ihre beziehungen zur hypophyse. Virchows Arch Pathol Anat. 1951. 320:437–458.
3. Kim ES, Kim IJ, Moon YJ, Na SK, Nam SY, Lee EJ, Kim KR, Song YD, Lim SK, Lee HC, Huh KB. Primary empty sellar syndrome: clinical and endocrinologic evaluation. J Kor Soc Endocrinol. 1997. 12:386–392.
4. Caplan RH, Dobben GD. Endocrine studies in patients with the "empty sella syndrome". Arch Intern Med. 1969. 123:611–619.
5. Brisman R, Hughes JEO, Holub DA. Endocrine function in 19 patients with empty sella syndrome. J Clin Endocrinol Metab. 1972. 34:570–573.
6. Neelon FA, Goree JA, Lebovitz HE. The primary empty sella: clincal and radiog raphic characteristics and endocrine function. Medicine. 1973. 52:73–92.
7. Jordan RM, Kendall JW, Kerber CW. The primary empty sella syndrome: analysis of the clinical characteristics, radiographic features, pituitary function and cerebrospinal fluid adenohypophyseal hormone concentrations. Am J Med. 1977. 61:569–580.
8. Lindholm J, Bjerre P, Riishede J, Gyldensted C, Hagen C. Pituitary function in patients with evidence of spontaneous disappearance of a pituitary adenoma. Clin Endocrinol. 1983. 18:599–603.
9. Jara-Albarran A, Bayort J, De Juan M, Benito C. Spontaneous partial empty sella. A study of 41 cases. Exp Clin Endocrinol. 1984. 83:63–72.
10. Bjerre P. The empty sella. A reappraisal of etiology and pathogenesis. Acta Neurol Scand Suppl. 1990. 130:1–25.
11. Gallardo E, Schachter D, Caceres E, Becker P, Collin E, Martinez C, Henriquez C. The empty sella: results of treatment in 76 successive cases and high frequency of endocrine and neurological disturbances. Clin Endocrinol. 1992. 37:529–533.
12. Ganguly A, Stanchfield JB, Roberts TS, West CD, Tyler FH. Cushing's syndrome in a patient with an empty sella turcica and a microadenoma of the adenohypophysis. Am J Med. 1976. 60:306–309.
13. Buchfelder M, Nistor R, Fahlbusch R, Huk WJ. The accuracy of CT and MR evaluation of the sella turcica for detection of adrenocorticotropic hormone-secreting adenomas in Cushing disease. Am J Neuroradiol. 1993. 14:1183–1190.
14. Bjerre P, Lindholm J, Videbaek H. The spontaneous course of pituitary adenomas and occurrence of an empty sella in untreated acromegaly. J Clin Endocrinol Metab. 1986. 63:287–291.
15. Findling JW, Tyrrell JB, Aron DC, Fitzgerald PA, Wilson CB, Forsham PH. Silent pituitary apoplexy: subclinical infarction of an adrenocorticotropin-producing pituitary adenoma. J Clin Endocrinol Metab. 1981. 52:95–97.
16. Wakai S, Fukuahima T, Teramoto A, Sano K. Pituitary apoplexy: its incidence and clinical significance. J Neurosurg. 1981. 55:187–193.
17. Nieman LK, Ilias I. Evaluation and treatment of Cushing's syndrome. Am J Med. 2005. 118:1340–1346.
18. Lee SH, Jeon HJ, Park SH, Kim SW, Park DJ, Park KS, Kim SY, Cho BY, Lee HK. Diagnosis of Cushing's disease by inferior petrosal sinus sampling (IPSS): evidence of false negative results. J Kor Soc Endocrinol. 1999. 14:483–492.
 XML Download
XML Download