

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Patients with adrenocortical carcinoma (ACC) present with evidence of excessive adrenal steroid hormone in approximately 60% of cases, in which rapidly progressing Cushing's syndrome with or without virilization is the most frequent presentation. Some patients experience an increase or a decline in cortisol production through the progression of their ACC. We report on an unusual case of a cortisol-producing ACC, and the patient presented with a decline in cortisol production, followed by an increase in cortisol production, through the progression of the tumor.
A 65-year-old woman who manifested with facial edema and weight gain was diagnosed with Cushing's syndrome, caused by cortisol producing ACC. The patient was treated with adrenalectomy. However, 8 months later, a metastatic hepatic tumor of recurred ACC was detected. At that time, the hormonal evaluation revealed that the liver mass did not produce any hormones. The patient was treated with metastatectomy. Four months later, a relapsed tumor was detected. Increased cortisol production was observed at that time. We speculate there was a change in the clonal dominance within the ACC and this change might cause such a difference. This is the first case report of ACC that showed variable hormone production during progression.
Figures and Tables
Fig. 1
Adrenocortical tumor at the time of diagnosis. Primary adrenocortical carcinoma is visualized at rightadrenal gland. This tumor corresponds to Fig. 4 (A) stage.
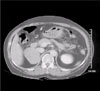
Fig. 2
Recurred tumor in liver. The CT scan shows metastatic hepatic tumor of recurred adrenocortical carcinoma. This tumor corresponds to Fig. 4 (E) stage.

Fig. 3
Tumors at the time of cortisol reproduction. Recurred tumors after hepatic metastatectomy are visualized at tumor bed (A) and in liver (B). These tumors correspond to Fig. 4 (J) stage.
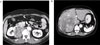
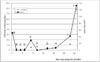
Fig. 4
Cortisol production in relation to tumor size. A, Diagnosis of adrenocortical carcinoma; B, No evidence of disease (NED) after right adrenalectomy; C, NED; D, NED; E, Recurrence of adrenocortical carcinoma in liver; F, NED after metastatectomy; G, Local recurrence at right adrenal gland tumor bed; H, Increase in tumor size; I, Tumor progression and invasion to liver; J, Detection of malignant effusion and lung metastases.
References
1. Carlo I, Barbagallo F, Toro A, Sofia M, Cordio S, Grasso G. Primary adrenocortical carcinoma and delayed liver metastasis: Is the surgery alone the right treatment? Hepatogastroenterology. 2004. 51:343–345.
2. Allolio B, Hahner S, Weismann D, Fassnacht M. Management of adrenocortical carcinoma. Clin Endocrinol. 2004. 60:273–287.
3. Kirschner L. Emerging treatment strategies for adrenocortical carcinoma: A new hope. J Clin Endocrinol Metab. 2006. 91:14–21.
4. Bertino J, Aaranson S, Brentani R, Cohen J, Dmitrovsky E, Houghton A, Scotto K, Skolnick M, Vogt P, Wang J, Woo S, Yahalom J. Encyclopedia of cancer. 2002. 2nd ed. California: Elsevier Science;165–177.
5. Damjanov I, Linder J. Anderson's pathology. 1996. 10th ed. Missouri: Mosby;513–524.
6. Mayer S, Cypess A, Kocher O, Berman S, Huberman M, Hartzband P, Halmos B. Uncommon presentations of some common malignancies. Case 1. Sequential paraneoplastic endocrine syndromes in small-cell lung cancer. J Clin Oncol. 2005. 23:1312–1314.
7. Hofle G, Gasser R, Lhotta K, Janetschek G, Kreczy A, Finkenstedt G. Adrenocortical carcinoma evolving after diagnosis of preclinical Cushing's syndrome in an adrenal incidentaloma. Horm Res. 1998. 50:237–242.
8. Hisamatsu H, Sakai H, Irie J, Maeda K, Kanetake H. Case report. Adrenocortical carcinoma with primary aldosteronism associated with Cushing syndrome during recurrence. BJU Int. 2002. 90:971–972.
9. Barzon L, Masi G, Fincati K, Pacenti M, Pezzi V, Altavilla G, Fallo F, Palu G. Shift from Conn's syndrome to Cushing's syndrome in a recurrent adrenocortical carcinoma. Eur J Endocrinol. 2005. 153:629–636.
10. Tan H, Thai A, Nga M, Mukherjee J. Development of ipsilateral adrenocortical carcinoma sixteen years after resection of and adrenal tumor causing Cushing's syndrome. Ann Acad Med Singapore. 2005. 34:271–274.
 XML Download
XML Download