INTRODUCTION
With the advancement of cancer treatment and early detection technologies, the number of cancer survivors is continually increasing. In 2011 in Korea, 220,000 patients were diagnosed with cancer[
1], representing a two-fold increase from 110,000 diagnoses in 2001. The cancer survival rate from 2007 to 2011 was 66.3%, a 22.3% increase compared to the survival rate of 44% from 1996 to 2000[
1]. This increase in cancer survival rate means that many cancer survivors will return to work during or after completing treatment[
2].
A cancer survivor is a person who has survived after overcoming cancer with severe difficulty or threat of life. The term refers to all individuals who have been affected by cancer from initial diagnosis and for the remainder of their lives[
3]. The increase in cancer survivors has been similar for military members. After amendment of the Military Personnel Management Act in 2007, members of the military who were previously discharged after cancer treatment were able to continue service[
4]. Considering the continually increasing cancer survival rate, the number of serving officers with cancer will continue to rise.
Career soldiers implement tasks in special environments that are different from those required of members of general organizations. The military profession requires a rigid life of strict discipline. Furthermore, frequently transferring shifts to remote areas and the frequent change of superior officers increase psychological stress. In addition, officers must always maintain readiness for duty and are constrained to living in certain areas[
5]. Officers with cancer will return to work following initial treatment to begin their lives as cancer survivors. They implement tasks that are both physically and psychologically intense under special conditions, such as service, training, and operations. During this process, it is expected that the officers with cancer will endure many difficulties. Thus, it is necessary to comprehensively evaluate difficulties faced by officers during the return to work experience. Return to work is an important part in the recovery of cancer survivors[
6,
7]. It solves economic problems[
2,
8], promotes social relationships in the workplace, and facilitates recovery toward a normal life[
8,
9]. Therefore, the ability to continue working is an important issue for the individual, his/her family, and society in general[
2]. However, many cancer survivors lose their regular source of income, their jobs, and even their social and psychological positions[
10]. Furthermore, even though these cancer survivors return to the workplace, it has been reported that they suffer difficulties due to cancer-related symptoms such as lack of attention, fatigue, pain, and depression[
11], negative attitudes toward cancer, and discrimination against cancer patients[
12] in the return to work process. A study on public perceptions of cancer and cancer patients showed that 23.5% of respondents wanted to avoid working with cancer survivors, and 50.7% of respondents indicated that, if they were diagnosed with cancer, they would not tell their coworkers[
13]. As such, the negative attitudes toward cancer influence people in their willingness to communicate their cancer diagnosis, which ultimately becomes a hindrance to cancer survivors' return to work.
International research on cancer survivors includes studies, mainly in the medical field, on factors that facilitate and hinder the return to work[
6], the experience of working following cancer treatment[
8,
11], employment after cancer diagnosis[
9], hospital-based work support interventions[
14], and improvement of the perception of cancer[
15]. However, studies thus far have been insufficient for informing nursing interventions. In other countries, researchers have studied the role of occupational health nurses in cancer survivors' return to work[
7], and how enlisted women with breast cancer balance cancer treatment and military service simultaneously[
16]. However, due to cultural and institutional differences in the perceptions or cancer treatment among career soldiers with cancer, the existing studies have limited applicability to the nursing of Korean career soldiers' return to work.
Only recently has research on cancer survivors' return to work in Korea begun to draw attention, and as domestic research is limited, most researchers have drawn comparisons with international research. Domestic studies have been mainly quantitative, and have focused on discrimination in the workplace[
12], the negative perception of cancer[
13], loss of employment and re-employment[
17], and work-related difficulties[
18]. Qualitative research remains insufficient, except for a study that analyzed the return to work experiences among breast cancer survivors[
19]. However, this study could not provide an understanding of survivors of other cancers. Few comprehensive studies have investigated the return to work experience among military officers with cancer. Such qualitative research could provide additional insights on cognitive and social factors as well as clinical processes[
10].
The transition process of cancer survivors, in which they conclude their role as patients and begin a new life as cancer survivors, could be a vulnerable state of crisis that could influence health conditions[
20]. Considering that the return to work is a process of recovery[
6,
7], nurses who are closest to the treatment trajectory of cancer survivors are in a unique position to provide support services with regard to vulnerable environments[
16]. Therefore, it is important that nurses devote attention to cancer survivors return to work after completing initial treatments. To provide adequate nursing for officers with cancer returning to work, qualitative research on the return to work among officers with cancer is required to gain a comprehensive understanding of their surrounding situations and environments.
Therefore, the purposes of this study were to comprehensively evaluate the difficulties faced by officers with cancer returning to work, to explore how they solved the problems and adjusted to the environment using the grounded theory approach based on symbolic interactionism, and to develop substantive theory that can explain these issues.
METHODS
1. Study design
We conducted a qualitative study based on experiential data to shed light on the return to work experience among officers with cancer. Strauss and Corbin's[
21] grounded theory approach for data collection and analysis was employed.
2. Setting and sample
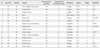
Participants were 15 cancer survivors who returned to work after completing treatment. Participants had at least 10 years of military service at the time of their diagnoses. They were selected using the Military Personnel System to identify the discharge state and workplace of cancer survivors who returned to work after cancer treatment between 2008 and 2012. In
Table 1 shows a summary of participants' demographic information. The average age of participants at time of diagnosis was 40.46±5.84 years. Among 15 participants, 12 were men and all were married. Cancer types included four with stomach cancer, four with colorectal cancer, one with gastrointestinal stromal tumor, two with breast cancer, one with brain tumor, one with lung cancer, one with liver cancer, and one with non-Hodgkin's lymphoma. On average, participants took 6.06±4.07 months after diagnosis before returning to work, and the time since diagnosis was 41.91±27.00 months. Seven people returned to work in a different workplace, and eight returned to the same workplace.
3. Ethical considerations
Ethical approval for the study was obtained from the Bio-Ethics Institutional Review Board of H University in Seoul (IRB approval number: HYI-13-087-1). Written consent was obtained from all participants, and it was indicated that all interviews would be recorded, kept confidential, and treated anonymously. Participants were told that they would not be negatively affected if they declined or cancelled participation, and that they had the option to discontinue participation at any time.
4. Data collection
Qualitative data were collected from September 2013 to April 2014 using in-depth interviews conducted by the first author with a semistructured interview. Participants were asked, "What was your experience of returning to work?" As the interview progressed, more specific questions were asked. During the interviews, the researcher observed and carefully noted facial expressions, attitudes, and gestures. One interview session took about 1~2 hours and the conversation was recorded using a handheld recorder. The researcher transcribed the interviews verbatim within 12 days. Each participant was interviewed 1~4 times at participants' workplaces, a nearby quiet coffee shop, or the researcher's office. During data collection, the researcher extracted significant concepts appearing in conversations through the process of continuous comparison and inquisition.
5. Data analysis
We coded data using Strauss and Corbin's[
21] grounded theory method. Data analysis was conducted in three steps.
First, in open coding, the data were analyzed according to line units by repeatedly reading transcribed interviews by researchers. To find concepts and name them, all the field notes, transcriptions, and theoretical notes were read and reviewed carefully, word by word, to clearly expose the meaning and thoughts contained in the interview. Concepts were found, labeled, and classified by meanings. Similar concepts were grouped into subcategories through continuous comparison, and similar subcategories were grouped into broader categories.
Second, axial coding was done, a process of linking subcategories with categories by re-assembling concepts that were disintegrated during the process of open coding. Based on the analyzed concepts and categories, the structures were analyzed in accordance with the paradigm model, and then, the process of change over time was analyzed. The questions "what are the difficulties suffered by officers with cancer in the process of returning to work?", "how do they solve the problems?", and "how do they adjust to the environment?" were analyzed through finding answers for why, how, where, and what consequences. Further, the relation with each category was identified using the paradigm model.
Third, in selective coding, which was the final stage of the analysis, a core category was derived to clearly represent the whole process of the study. The core category emerged from this repetitive trial-and-error process of analysis. When the core category was determined, the process that characterized the core category was analyzed.
6. Ensuring the quality of the results
For qualitative research assessment of the findings, credibility, fittingness, auditability, and confirmability, as proposed by Sandelowski[
22], were used to ensure the quality of results. Assessment of the researcher's capability to maintain relationships of trust with participants, gained through more than 20 years of experience as an army nurse was used to satisfy credibility. The researcher attempted to enhance credibility of the study by exploring participants' various experiences through the same interview questions, transcribing the participants' speech as they spoke, and then by obtaining feedback from the co-researcher. In addition, the researcher tried to achieve thorough analysis of the primary data by adding explanations and descriptions, including both typical and atypical elements of the data. Fittingness is related to diversity, limitations, universality, and depth of situations. In this study, the researcher attempted to enhance fittingness by describing the core category and each phase of the adjusting process in-depth. Auditability is the degree to which readers can track the researcher's process of decision-making and the results of the research. For this purpose, the researcher described participant selection, data collection, and analysis procedures in as much detail as possible. Furthermore, in order to obtain relevance between the induced categories and actual data, the statements of participants are included in the relevant categories. As such, it is deemed that by securing credibility, fittingness, and auditability, the experiences and viewpoints of participants are maximally reflected and prejudice of the researcher is minimized to establish confirmability.
DISCUSSION
In Korea, officers with cancer have been able to serve continuously since 2007. Therefore, it is important to understand how cancer affects officers serving in the army. This study was the first in Korea in which an investigation was done of the return to work experience of military officers with cancer, and to explore how they endure negative reactions and how they adjust to maintaining a balance between work and treatment. The results of this study make a substantial contribution by describing the process of enduring difficulties and adjusting to work among officers with cancer who, after completing the initial treatment and during their recovery, they return to work with high physical demands.
The core category of return to work experiences among officers with cancer was found to be living a new life after enduring difficulties. It was identified as having four phases which the officers had to undergo to adjust to their duties: chaos, positive thought formation, behavior practices, and reformation.
The core process of enlisted women with breast cancer was, in an earlier study, found to be balancing demands and expectations. This is somewhat different from the core category of the present study. This may be because most participants in the present study focused on healthcare in order to prevent recurrence and were trying to reduce the burden of their duties. However, in Wilmoth's[
16] study, participants were all women with childcare issues in addition to their career issues and treatment, and thus 'balancing demands and expectations' appears to be a reasonable core construct.
Participants' return to work was important in terms of economic concerns, was a process of recovery, provided psychological security, and acted as a diversion. The findings were consistent with previous studies[
2,
7,
19,
23,
24]. However, job satisfaction and recovering a sense of existence were important concepts revealed in this study. This outcome may be the result of satisfaction with the rank and position of each participant who had served in the army for at least 10 years.
In relation to the return to work, participants had not received practical information or support from medical practitioners. Although participants returned to work after initial treatment, continuous fatigue, depression, and pain made it difficult for them to implement required duties. A lack of information and support from the medical team and effects of the cancer and treatment, which were identified as issues in this study, is consistent with issues identified in previous studies[
11,
15,
23]. Therefore, it is necessary to instruct medical practitioners to maintain a reliable relationship with cancer survivors and to provide information by intervening at points of decline in physical function and the capacity of survivors to be active[
25].
Participants changed their priorities at work, as they thought balancing work and health care was important to return to the work performance they had displayed before being diagnosed with cancer. This change in priorities among cancer survivors was reported in other qualitative studies[
7,
23,
25]. The reasons for this shift in priorities, however, differed between studies. Some individuals placed more emphasis on giving themselves more personal time in relation to work due to fear of recurrence and uncertainty about life[
7], wanting to use their time meaningfully, and wanting to be a better person[
23]. In this study, in order to maintain a balance between health recovery and work performance, participants made adjustments to their work by reducing work burdens and minimizing work stress at the initial stage of returning to work. In addition, they maintained a healthy diet, exercised regularly, and conducted continuous management including regular examinations to prevent recurrence.
Among the participants, 12 (80%) were relocated after the cancer diagnosis. Participants who returned to the same workplace received substantial support with night duties and outdoor training from commanders and colleagues with whom they had worked previously. However, when participants were relocated, the coworkers of the new workplace had mostly negative perceptions about the work ability of participants. Negative reactions may have occurred because military activities require highly demanding physical activities, and it would be difficult to conduct normal activities immediately following treatment[
16]. This is consistent with the finding of a Korean study that 56.1% of participants agreed that the work ability of cancer patients would be reduced even after successful treatment[
13].
Coworkers in the workplace expected that officers with cancer would implement duties normally after some time had passed following their return and subsequent health recovery. However, in reality, there were more cases in which considerable time had passed following treatment completion and cancer-related fatigue continued to affect participants' implementation of duties. Previous studies[
2,
6,
7] noted that it is necessary for cancer survivors to accept their limitations in work performance capacity and to talk to supervisors and colleagues frankly about the facts regarding their cancer recovery. As people generally lack knowledge and understanding about cancer and easily forget that these individuals are patients, sincere communication is necessary to discuss cancer survivors' health status and to share healthcare experiences. Participants considered guaranteeing their attendance at regular examinations and other treatments to be important. This is consistent with the findings from a study on breast cancer survivors among immigrants and ethnic minorities[
9], which reported that work hour flexibility and adjustment have a positive impact on their return to work experience. Therefore, it is important to guarantee conditions for treatment in order to monitor their present health status and manage recurrence prevention through regular examinations.
The return to work experience of the military officers and that of civilians are similar in many regards. However, military officers differ in that their workplace changes frequently, physical fitness testing is required, and they have to perform specific duties and field training. Thus, thorough healthcare, physical fitness management, and enhanced social support is required.
Based on the discussion so far, it is possible to propose a set of nursing interventions applicable to each phase of the return to work among officers with cancer. In the chaos phase, it is necessary to identify patients' preparedness for a change of duties and roles and to understand what support is needed and what is expected before the transfer[
20]. In the positive thought formation phase, participants should understand that they can discover life aims through this experience, and they should be encouraged by the opportunity for growth[
26]. In the behavior practices phase, if the patient is in the middle of treatment or within 1 year of completing treatment, adverse effects of exercising or exercise-related injuries can hamper the treatment[
27]. Therefore, it is necessary to provide evidence-based information or connect them with experts for advice. Further, as it is not easy to change eating habits or control weight, they tend to postpone weight control until after surgery or radiation and anticancer treatments[
28]. Thus, life habits, such as diet, must be properly controlled. In the final phase, it is necessary for them to accept prioritizing personal time over work to improve coping ability against cancer[
7,
10,
23]. In addition, individuals should be praised through their willpower to promote the practice of new health-related habits.
There are some limitations in this study. As a qualitative study, caution should be exercised in interpreting the results. In this study, data were analyzed for 15 career soldiers with cancer with at least 10 years of military service. When applying the research findings to other cancer survivors, the social and cultural background of Korea should be considered. Despite these limitations, various stages, treatments, and diagnoses of the illness were sufficiently considered, as well as the rank and gender of the patients.
CONCLUSIONS
In this study a substantive theory was developed by revealing military officer cancer survivors' endeavor to maintain new healthy habits and improve relationships with people around them and the importance of social support systems in order for officers with cancer to live a new life after enduring difficulties. The most difficult aspect of the process of returning to work was the negative perceptions of cancer among coworkers. The most worrying issue was fear of recurrence, and the top priority was healthcare. Therefore, along with managing physical symptoms, a psychosocial approach is required for officers with cancer when they return to work.
As the return to work experiences of officers with cancer were different depending on the phases, the study results suggest that differentiated systematic nursing should be applied to cancer survivors with consideration to each individual's context and intervention situations at each phase. By illuminating the experiences of return to work among officers with cancer, this study will be helpful in developing a more effective nursing intervention by enhancing the perspectives and insights of practitioners.
Based on the findings, the following considerations are suggested. First, it is necessary to develop tools that can measure the degree of preparedness for return to work among officers with cancer and their return phase. Second, in order to identify the factors related to return to work in greater detail, a focus group study would be necessary targeting cancer survivors, managers, and medical practitioners.


 PDF
PDF ePub
ePub Citation
Citation Print
Print



 XML Download
XML Download