METHODS
1. Design
This study is the non-equivalent control group pre-post test design which compares the knowledge and behaviors related to dental health, perceived benefits and barriers, self-efficacy and plaque control scores between the experimental group for which the dental health program with the mothers' involvement was applied and the control group to which the knowledge related to dental health was provided through the brochures.
2. Samples
For subjects of this study, the researcher conveniently selected two places by reviewing possibility of carrying out dental health programs with mothers' involvement in elementary schools located in K district. One of the two elementary schools was designated as experimental group and the other as the control group wherein all students belonging to 5th grade in both schools were the subjects.
For the sample size required by this study, it was computed that 20 subjects per group would be needed as a result of using Power and Sample Size program based on the results of a two-sided test where a=.05 and 1-β=0.8 for the independent sample t-test (
Dupont & Plummer, 1990), which was based on data (mean difference between two groups=16.7, standard deviation=18.5) from research (
Son, 2003) about the effects of dental education program on plaque index. Total of 50 children were subjects of this study wherein experimental group had 26 children and control group had 24 children without any dropouts along the way.
3. Development and application of dental health programs with mothers' involvement
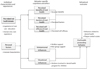
For the conceptual framework of this study, variables were selected through previous papers based on the revised health believe model by Pender (
1996), which formed the main contents of the program (
Figure 1).
For "individual characteristics and experiences," related behaviors in the past and personal factors were considered. Accordingly, this study measured its data by applying past behaviors related to oral health (oral care education, dental clinic visit experience) and children's personal factors (general characteristics).
For "behavior-specific cognitions and affect," factors included perceived benefits of behavior, perceived barriers of behavior, perceived self-efficacy, interpersonal influences, and situational influences. Interventions that increase benefits and self-efficacy while reducing barriers were applied through dental health programs with mothers' involvement.
Interpersonal influences refer to interactive effects between persons and the effects of interpersonal relationship are a perception of the behaviors, beliefs, and attitudes of others. The primary source of factors influencing interpersonal relationships regarding the promotion of health includes family (parents and siblings), peer group, and healthcare provider. In addition, such interactive effects are comprised of norms (significant expectations toward others), social support (sentimental support, instrumental support), modeling (vicarious learning while observing others participating in certain action), and others. In this aspect, this study applied a dental health program wherein reinforcements through supports and complements from mothers of children in the experimental group, homeroom teachers, and health teachers, in addition to influence from correct oral health behaviors from peers, were provided.
For situational influences, individuals may expedite or hinder behaviors depending on how they perceived and became aware. Situations for good conduct of health behaviors must be interesting and attractive. Situational influences in revised health believe model had been re-perceived to have direct and indirect effects on health behaviors. Accordingly, a dental health program with a mother's involvement was applied to the experimental group whereas brochures and dental hygiene materials related to oral health were provided to the control group.
As shown, "individual characteristics and experiences" and "behavior-specific cognitions and affect" interacted and resulted in the appearance of health-promoting behaviors, which were a "behavioral outcome." Subsequently, this behavioral outcome was measured by oral health behaviors and the O'Leary plaque index.
4. Measurements
1) Knowledge related to dental health
We used measurement tool which was developed by Ahn and Yi (
2010) by revising the tool that was used for measuring dental health knowledge in elementary students by Lee and Park (
2000). It is comprised of total of 11 questions in which 1 is given for each question answered correctly and 0 for incorrect answers for a total of 11 points wherein higher the score, higher the knowledge in dental health. In a research by Ahn and Yi, the reliability was Cronbach's α=.70. In this study, the converted scores ranged between 45.45-100 (pre test) before and 72.72-100 (post test).
2) Perceived benefits
Among the measuring tool developed by Ahn and Yi (
2010) by revising the tool used by Lee and Park (
2000) to investigate beliefs related to children's oral health, we used benefits of dental health. It is comprised of 7 questions which are responded in scales from 'most definitely (5)' to 'not at all (0)'. Higher score means higher perceived benefits. In this study, reliability was Cronbach's α=.70.
3) Perceived barriers
Among the measuring tool developed by Ahn and Yi (
2010) by revising the tool used by Lee and Park (
2000) to investigate beliefs related to children's oral health, we used barriers of dental health. It is comprised of 5 questions which are responded in scales from most definitely (5) to not at all (1). Higher score means higher perceived barriers. In this study, reliability was Cronbach's α=.71.
4) Perceived self-efficacy
We used measuring tool developed by Ahn and Yi (
2010) to measure self-efficacy related to children's dental health. It is comprised of 8 questions which are responded in scales from most definitely (5) to not at all (1). Higher the total score signifies increased perceived self-efficacy. Higher total score signifies higher perceived self-efficacy. In a research by Ahn and Yi, reliability for perceived self-efficacy was Cronbach's α=.81. In this study reliability was Cronbach's α=.87.
5) Behaviors related to dental health
We used measuring tool revised and developed by Ahn and Yi (
2010) to measure dental health behaviors of elementary school students. This tool is comprised of total of 13 questions that ask for ordinary dental health behaviors, which is responded by 4 point scale for each as always, frequently, sometimes and never. Higher score signifies more preferable ordinary dental health behavior. In a research by Ahn and Yi, the reliability was Cronbach's α=.81. In this study reliability was Cronbach's α=.82.
6) Plaque control scores
Plaque control scores measured by using O'Leary plaque index for degree of stain of 4 sides of the teeth (root area, top area, anterior area, posterior area) when all teeth are dyed with teeth stainers (
Jo, 2010). In this study, we used teeth stainers and O'Leary plaque index to measure plaque control score. Product name of teeth stainer used in this study and evaluation method of plaque control score are as follows.
Disclosing tablet: Product name is Red-Cote Tablet (Sunstar Americas-GUM, Chicago, U.S.A). It reacts with layer of bacteria formed on tooth surface and dyes the tooth red.
Plaque Control Scores: This is score computed from quantifying whether plaque has built up and stained or not when all teeth are dyed with the stainer. All teeth are subject to this treatment and whether or not plaque build-up exists is evaluated for each of the 4 areas. After evaluating each tooth with plaque score of 0-4, O'Leary plaque index is obtained by percentage from dividing the total score by number of tooth sides inspected, which is then subtracted from 100. Higher the number signifies better plaque control score, which means tooth brushing is properly done. Evaluation method for quantification is as follows (Eom, Jeong, & Park, 2009).
Criter ia for Plaque Inspection
In this study, ranges for plaque control scores were 13.50-89.30 points for before and 16.10-98.20 points for after. Moreover, matching rate between principal researcher and research assistant was 99.8% (
p<.001). Generally, interrator reliability 85.0-95.0% is considered appropriate and results of this study accorded to this standard as well (
Chang & Kim, 2007).
5. Procedure
Period of data collection for this study lasted from November 2010 until December and detailed description is as follows. First, after receiving approval our university's Institutional Review Board (approval No.: 10-26), we received agreement from principals, homeroom teachers and health teachers of the subject elementary schools before starting the experiment. Moreover, after explaining the objective and contents of this experiment and sending out explanation letter and agreement form to subject children and their mothers, we received written agreement from children and mothers who voluntarily agreed to their participation.
Afterwards, we proceeded with previous research regarding measurement variables of experimental group and control group. Then we provided the control group with oral products, educational materials on dental health, tooth brushing diary that contains tooth brushing record table while for experimental group, we applied dental health program with mothers' involvement (
Figure 2) for 5 weeks. Lastly, we gathered data by conducting post-investigation regarding measurement variables from the experiment and control groups.
Research roles were comprised of 2 professors of child health nursing as researchers and 3 nursing undergraduates as research assistants. Researchers had continuous discussions for general planning and operation of program with mother's involvement. Researcher with experience in carrying out dental health program offered general advice for construction and management of the program. Other researchers directly participated in actual operation of program in general. Detailed guidance was provided regarding methods of tooth brushing, tongue cleaning and dental flossing through training with research assistants. Subsequently, research assistants were able to provide consistent demonstrations and guidance to elementary school students.
6. Data analysis
All data were analyzed using by using SPSS 18 program. General characteristics of experiment and control groups were analyzed using descriptive statistics such as frequency, percentage and others; general characteristics between the two groups and homogeneity verification of dependent variables were analyzed through χ2-test and t-test, and differential analysis between experimental group with application of dental health program with mothers' involvement and the control group was analyzed by using paired t-test.
DISCUSSION
This research was conducted to study the effects on behaviors that improve dental health in children by developing dental health program with mothers' involvement.
The results of this study showed that dental health knowledge and behavior was higher and significantly increased for experimental group that participated in dental health program with mothers' involvement compared to control group. Such results support results of previous researches (
Ahn & Yi, 2010;
Lee & Park, 2000;
Son, 2003) which showed that application of dental health programs for children is effective for improving dental health knowledge and behavior and we believe that dental health program with mothers' involvement in this study is also effective in improving dental health knowledge and behavior.
Results of this study was similar to study results of Hartomo, Lamvri, and Helderman (
2002) that reported that dental health knowledge significantly increased in children who received education on tooth brushing under teacher's supervision and to study results of Zahra (
2010) that reported that tooth brushing frequency is high for children who received dental health care and supervision from their mothers and that dental health condition behavior are high. We believe that it is due to this study also applying practice oriented individual lesson program under researcher's guidance. Especially, the approach that allowed individual guidance to tooth brushing at home under mothers' supervision is thought to have significantly increased both knowledge and behavior of dental health.
In this study, we implemented dental health program with mothers' involvement which could be continued not only in school for dental health education but also at home as a method to increase dental health knowledge and behavior in children. As shown in previous study (
Min & Min, 2010), school's dental health education may increase children's knowledge in dental health but difficulty exists in increasing their behavior. Moreover, since schoolage children are at times of being greatly influenced by their parents, effective behavioral change can only be expected when health education is extended to their homes as well. We believe that this is why operating an integrated and practical dental health program through practice oriented individual guidance and school dental health education under researcher's supervision together with involvement of mothers as the key person at home just like in this study not only increased dental health knowledge in children but also improve their behavior as well.
Moreover in this study, we regularly provided dental health information through short message service (SMS) texts twice a week aside from brochures as a method to increase dental health knowledge for mothers. Internet cafe was also established so cafe information was shared with mothers at every home. In the Internet cafe, we created open cyber space in which mothers and children can participate with interest at home by uploading dental health related videos and images for learning with children. In addition, we made it possible for children and mothers to check anytime by uploading reviews and activity photos of dental health program carried out weekly, especially children's photos of plaque staining by program session.
We also provided tooth brushing diaries so that children's dental health behavior can be practiced at home as well, which induced proactive participation of mothers by allowing them to check and support their children's dental health behaviors. We believe that results of developing and managing such program allowed for significant increase in both knowledge and behavior of children in relation to dental health. Moreover, we support the study results of Lee (
2010) and Jun, Choi, and Cho (
2009) that reported that higher the level of dental health knowledge of mothers, higher the dental health behaviors of their children, which suggests that various approaches that can increase dental health knowledge of mothers should be carried out in order to increase the ones of children as well.
Therefore, application of not only knowledge education but also direct demonstration, practice oriented individual lessons and other various education methods while increasing opportunities for mothers' involvement is thought to be recommended for future dental health program of elementary students in the future. For constraints, brochures and sending SMS texts to increase mothers' dental health knowledge and behavior were only able to provide one-sided dental health knowledge. In addition, running an Internet cafe was a limited approach method for mothers of families that do not use computers often. Subsequently, web-based program using smart phones should be developed as one of methods to overcome such problems and studies to examine its effects will be needed to be conducted in the future.
Second important result was that perceived self-efficacy related to dental health of experimental group that dental health program with mothers' involvement significantly increased while there was no change to perceived benefits and barriers. Such result partially resembles the study results of Ahn and Yi (
2010) that applied dental health program for 6th graders in which there was significant increase in perceived benefits and self-efficacy for group that participated in dental health program but no difference with barriers. Moreover, our results were similar to the study results of Hong (
2006) that researched on 4th to 6th graders which showed main variable that explains the behavior of children's health improvement to be self-efficacy and to the study results of Yi and Hyun (
2009) in which it showed that higher dental health knowledge and belief and better behavior were resulted as self-efficacy on dental health increased.
In addition, results of applying dental health program with mothers' involvement by allowing children to care for their dental health themselves by using support through reinforcements and disclosing tablets were similar to the study results of Lee and Park (
2000) that showed positive increase in benefit and importance among dental health principles for children who received much social reinforcements from peer group.
In this study, reinforcement stickers were provided by researchers, homeroom teachers and health teachers when children voluntarily brushed their teeth, effectively removed plaque and took action for dental health during their school life. Moreover, additional reinforcement stickers were given when they honestly carried out the given assignment of self-recording their tooth brushing diary after brushing their teeth even during weekends with no classes or after school. Apart from this, attention was paid so that dental health behavior could be continued at home as well. In other words, reinforcement stickers were given under same criteria as in school by providing mothers with reinforcement stickers and guide to using disclosing tablets and guidance to correct tooth brushing technique after meals to control plaque was implemented while children were to be given support.
During group tooth brushing after lunch, individual guidance for correct tooth brushing technique was carried out so that children can remove the stain themselves after observing red-stained teeth due to poor brushing of teeth. When we take a general look at the results of this study and methods of intervention, it can be viewed that they provide the evidence for deduction that support from mothers, homeroom teachers and health teachers who are influential to children affects perception and emotions related to dental health. Among these, we believe that dental health program with mothers' involvement is effective in improving perceived self-efficacy related to children's dental health. On the other hand, there were no significant changes before and after program participation for perceived barriers related to dental health.
Such result coincided with study results of Ahn and Yi (
2010) and Ahn et al. (
2009). However, we think that lack of significant change was due to some questions of the tool for measuring perceived barriers related to dental health being inappropriate for measuring barriers related to children's dental health. As such, it seems that improvement in dental health behavior of children is greatly influenced by self-efficacy, and reinforcement and support from people influential to them. Thus, in the future, there is a need to develop programs for enhancing general dental health with reinforced perception and emotions related to dental health and prove their effectiveness. Moreover, we will have to develop a tool which could accurately measure barriers related to children's dental health and confirm its effects after application.
Lastly, experimental group that participated in this program had higher plaque control score compared to the control group, which increased significantly. Such result coincided with study results of Choi and Park (
2008), Eom et al. (
2009) and Son (
2003) that investigated on plaque control score by applying O'Leary Plaque Index evaluation method. Moreover, results were similar to previous researches (
Chae, Kim, Jang, Kim, & Lee, 2009;
Eom et al.;
Jo, 2010) that showed that plaque control score increased through continuous and repetitive education while one-time education had no improvement effects of the scores. Even if frequency of brushing teeth among dental health behaviors increases, plaque that induces dental diseases is not completely removed unless correct tooth brushing technique is carried out. Plaque is the leading cause for dental caries and periodontal diseases and one of the easiest methods to care for this is correct brushing of teeth. However, correct tooth brushing technique needed for removal of plaque cannot be learned by one-time education. In other words, systematic and step-by-step repetitive education until the child fully learns the correct technique is needed (
Eom et al.;
Kim et al., 2009). Despite these difficulties, not only dental health behaviors of children in experimental group in this study increased but also plaque control score significantly increased as well.
Such results support the effectiveness of repetitive learning for formation of correct tooth brushing technique by implementing visual motivation through children directly observing bacterial layer that remains on tooth surface by using stainer after eating school lunch and having individual lessons for teeth that are difficult to brush by themselves. We especially believe that direct experience of trying out oral care supplies (floss, inter-dental brush, tongue cleaner) and strategy of carrying out video education on their usage and providing individual guidance together were effective. Moreover, disclosing tablets together with its manual were provided so that children's plaque control status can be checked easily even at home.
In addition, we allowed mothers to check children's plaque control condition any time by sending photos of children's stained teeth that were taken while carrying out the program in school via SMS text image service every week. Also, as the final event for the program, we conducted photo contest called 'plaque test with mummy and daddy' to build an environment that allows all family members including children of experimental group to actively engage in plaque control.
Likewise, average plaque control score before participating in dental health program with mothers' involvement was 40.03 points. When compared to average of 38 points for plaque control score obtained from Eom et al. (
2009) in which the study was conducted for walk-in patients of preventive dental clinic, it is of similar level and signifies poor plaque control. After program participation, plaque control score of experimental group increased to average of 77.66 points with average of 37.63 point increase compared to pre-participation score, which shows statistically significant difference. This was similar to results of Eom et al. where in plaque control score increased to average of 70 points after completion of education. Above all, in this study, the improvement range of plaque control score being average of 37.62 points was higher than increase of 32 points in previous studies. Therefore, this suggests that running active and practice oriented dental health program wherein parents and children can participate together not only in school but also at home by using dental stainers can contribute to improving plaque control for children's dental health care.
Previous studies limitedly discussed mothers' participation in the said aspect although many dental health programs have been mainly applicable to children. However, this study developed and aplied methods for mothers to easily participate in together with their children. Moreover, the results of applying this program in which children's nurses and health teachers encouraged and widened mothers' participation confirmed that mothers' involvement is effective in improving oral health in elementary school students. In other words, this study suggests that such nursing intervention is significant since the application of an oral health program with mothers' involvement is effective in improving oral health in elementary school students.
Therefore, a dental health program with mothers' involvement could be utilized as a hands-on guideline for health teachers who are in charge of children's dental health education which is related to nursing practices. Moreover, reduced dental loss and dental expenses can be expected through an application of this program in actual practice in which management of dental caries in elementary school students are focused upon. Accordingly, oral health program with mothers' involvement can be considered as a cost-effective nursing intervention approach. In addition, the oral health care with mothers' involvement that has been developed through this study can also contribute to nursing intervention in promoting children's oral health to be applied not only for school-age children but also pre-schoolers. Furthermore, the study can be utilized in developing programs for a wider range of children and parents of diverse age groups.
Restrictions for this study included the usage of passive methods such as brochures, telephone counseling, and Internet cafe to increase the participation of mothers, and the fact that test subjects were higher grade level students among school-age children. Therefore, we believe that there is a need to develop diverse programs that take into consideration children's different developmental stage and that can increase participation of mothers for enhancement of children's dental health in the future with studies that verify their effects. Another restriction was that changes and long-term effects according to progress in time could not be verified since the program was only short-term. Accordingly, studies on verifying long-term effects after application of a dental health program seemed to be needed. Therefore, we believe there is a need for research on proving long term effects after application of children's dental health program.
CONCLUSION
This study viewed that there is a need for preventive management for dental caries as urgent project for enhancement of dental health in elementary school students. In regards to this, we implemented dental health program with mothers' involvement that comprised of dental health education, reinforcement through providing reinforcement stickers, support, individual tooth brushing lessons using disclosing tablets and increasing self-efficacy through repetitive learning both in school and at home over the course of 5 weeks centered on the researcher and mothers. As a result, we were able to confirm the effectiveness of this program through significant increase in dental health knowledge, perceived self-efficacy, dental health behavior and plaque control scores for experimental group that participated in dental health program with mothers' involvement.
Especially, education using video lectures, various activities and practical hands-on experience that can induce interest rather than lecture-type dental health education can be said to be more effective in increasing dental health knowledge and behavior in children. In addition, strategy of carrying out dental health behaviors such as individual tooth brushing lessons not only in school but also at home under adult supervision is very significant in that it can improve both dental health knowledge and behavior in children. Moreover, implementation of reinforcement such as reinforcement stickers and awards for excellent children in dental health is influential and support from meaningful people (mother, homeroom teacher, health teacher, peer group) is effective for improving dental health behavior and perceived self-efficacy in children. Lastly, practical hands-on individual education and repetitive learning using disclosing tablets can easily be carried out in school and at home and are effective not only for improvement of plaque control scores but also increasing perceived self-efficacy.
As discussed above, this study systematically proposes that perceived benefits, perceived barriers, self-efficacy, and support related to oral health program with mothers' participation increase oral health-promoting promoting behaviors. In addition to nursing practices, oral health program with mothers' involvement in which children's nurses and health teachers encouraged and widened mothers' participation is effective in promoting oral health of elementary school students.


 PDF
PDF ePub
ePub Citation
Citation Print
Print






 XML Download
XML Download