

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The purposes of this study were to identify the prevalence of postprandial hypotension (PPH) and risk factors for PPH in Korean elderly people.
Methods
A cross-sectional descriptive study was conducted with community dwelling and nursing home residents. The blood pressure of 162 adults aged 65 yr or older was measured before meal as a baseline and then at 15 min intervals from immediately after the meal through 90 min after the meal. Descriptive statistics and logistic regression with the SPSS WIN 14.0 program were used to analyze the data.
Results
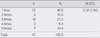
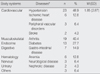
The prevalence of PPH was 29% and the PPH occurred immediately after the meal continuously through 90 min after the meal. The biggest drop in systolic blood pressure occurred at 45 min after the meal. Risk factors for PPH were age, base line systolic blood pressure, and presence of cardiovascular disease.
Figures and Tables
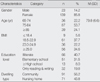


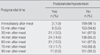
Table 5
Comparison of After Meal Systolic Blood Pressure with Baseline Systolic Blood Pressure (N=162)

References
1. Aronow WS, Ahn C. Association of postprandial hypotension with incidence of falls, syncope, coronary events, stoke, and total mortality at 29-month follow-up in 499 older nursing home residents. Journal of the American Geriatrics Society. 1997. 45:1051–1053.
2. Fisher AA, Davis MW, Srikusalanukul W, Budge MM. Postprandial hypotension predicts all-cause mortality in older, low-level care residents. Journal of the American Geriatrics Society. 2005. 53:1313–1320.
3. Gladstone SA. Cardiac output and related function under basal and postprandial condition. Archives of Internal Medicine. 1935. 5:533–546.
4. Grodzicki T, Rajzer M, Fagard R, O'Brien ET, Thijs L, Clement D, et al. Ambulatory blood pressure monitoring and postprandial hypotension in elderly patients with isolated systolic hypertension. Journal of Human Hypertension. 1998. 12:161–165.
5. Jansen RW. Postprandial hypotension: Simple treatment but difficulties with the diagnosis. The Journal of Gerontology. 2005. 60:1268–1270.
6. Jansen RW, Lipsitz LA. Postprandial hypotension: Epidemiology, pathophysiology, and clinical management. Annals of Internal Medicine. 1995. 122:286–295.
7. Jones KL, MacIntosh C, Su YC, Wells F, Chapman IM, Tonkin A, et al. Guar gum reduces postprandial hypotension in older people. Journal of American Geriatrics Society. 2001. 49:162–167.
8. Kawaguchi R, Nomura M, Miyajima H, Nakaya Y, Mouri S, Ito S. Postprandial hypotension in elderly subjects: Spectral analysis of heart rate variability and electrogastrograms. Journal of Gastroenterology. 2002. 37:87–93.
9. Kohara K, Jiang Y, Igase M, Takata Y, Fukuoka T, Okira T, et al. Postprandial hypotension is associated with asymptomatic cerebrovascular damage in essential hypertensive patients. Hypertension. 1999. 33:565–568.
10. Kohara K, Uemura K, Takata Y, Okura T, Kitami Y, Hiwada K. Postprandial hypotension: Evaluation by ambulatory blood pressure monitoring. American Journal of Hypertension. 1998. 11:1358–1363.
11. Causes of Death. Korea National Statistical Office. 2006. 10. 20. Retrieved June 30, 2008. from
http://www.kosis.kr/html/InterStatic/staticCount.jsp.
12. Kuipers HM, Jansen RW, Peeters TL, Hoefnagels WH. The influence of food temperature on postprandial blood pressure reduction and its relation to substance P in healthy elderly subjects. Journal of American Geriatrics Society. 1991. 39:181–184.
13. Le Couteur DG, Fisher AA, Davis MW, McLean AJ. Postprandial systolic blood pressure responses of older people in residential care: Association with risk of falling. Gerontology. 2003. 49:260–264.
14. Lipsitz LA, Nyquist RP Jr, Wei JY, Rowe JW. Postprandial reduction in blood pressure in the elderly. The New England Journal of Medicine. 1983. 309:81–83.
15. Lubart E, Segal R, Baumoehl Y, Matron M, Leibovitz A. Postprandial hypotension in long-term care elderly patients on enteral feeding. Journal of the American Geriatrics Society. 2006. 54:1377–1381.
16. Health Disease Information. National Health Insurance Corporation. 2008. 05. 16. Retrieved June 30, 2008. from
http://www.nhic.or.kr.
17. Oberrman AS, Gagnon MM, Kiely DK, Nelson JC, Lipsitz LA. Autonomic and neurohumoral control of postprandial blood pressure in healthy aging. Journal of Gerontology. 2000. 55:M477–M483.
18. O'Donovan D, Feinle C, Tonkin A, Horowitz M, Jones KL. Postprandial hypotension in response to duodenal glucose delivery in healthy older subjects. The Journal of Physiology. 2002. 540:673–679.
19. Puisieux F, Bulckaen H, Fauchais AL, Drumez S, Salomez-Granier F, Dewailly P. Ambulatory blood pressure monitoring and postprandial hypotension in elderly persons with falls or syncopes. Journal of Gerontology. 2000. 55:M535–M540.
20. Sidery MB, Cowley AJ, MacDonald IA. Cardiovascular response to a high fat and a high carbohydrate meal in healthy elderly subjects. Clinical Science. 1993. 84:263–270.
21. Smirk FM. Action of a new methonium compound (M & B 2050A) in arterial hypertension. Lancet. 1953. 1:457.
22. Smith NL, Psaty BM, Rutan GH, Lumley T, Yanez D, Chaves PH, et al. The association between time since last meal and blood pressure in older adults: The cardiovascular health study. Journal of the American Geriatrics Society. 2003. 51:824–828.
23. Vaitkevicius PV, Esserwein DM, Maynard AK, O'Connor FC, Fleg JC. Frequency and importance of postprandial blood pressure reduction in elderly nursing-home patients. Annals of Internal Medicine. 1991. 115:865–870.
24. Vloet LC, Smits R, Jansen RW. The effect of meals at different mealtimes on blood pressure and symptoms in geriatric patients with postprandial hypotension. The Journals of Gerontology. 2003. 58:1031–1035.
25. Yokota T, Kamata T, Mitani K. Postprandial cerebral ischemia. Stroke. 1997. 28:2322–2323.
26. Yu SJ, Song MS, Kim HS. A study on the prevalence and risk factors of postprandial hypotension among the community-dwelling aged. Journal of Korean Academy of Fundamentals of Nursing. 2002. 9:434–444.
 XML Download
XML Download