

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diabetes mellitus (DM) is a metabolic disorder, of which the number of patients is rapidly increasing worldwide due to several conditions such as aging, westernization, and increasing prevalence of obesity and physical inactivity every year, and particularly, it is one of the major treatment-requiring diseases nowadays [1]. Diabetic peripheral polyneuropathy (DPP), one of the common complications of DM, predisposes the patient to foot ulcers or amputation [2]. DPP is associated with various symptoms including paresthesia, numbness, pain, muscle weakness, and loss of reflexes. The prevalence of DPP is underreported due to the lack of consistent diagnostic standards [3, 4]. Several objective methods have been used for screening and early detection of peripheral polyneuropathy including the Michigan neuropathy screening instrument (MNSI) [5], vibration perception threshold test [6], tactile tests performed with monofilament [7], quantitative pressure threshold test [8], and nerve conduction velocity (NCV) examinations [2,3].
The pathophysiology of diabetic neuropathy includes several factors such as metabolic, vascular, autoimmune, oxidative stress, and neurohormonal growth-factor deficiency [3]. Recent studies have reported that oxidative stress may apparent in pathology associated with metabolic syndrome and neurodegenerative disease and suggested that serum gamma-glutamyl transferase (GGT) may be an early marker of oxidative stress [9,10]. Therefore, we investigated the relationships between DPP and serum GGT as a marker of oxidative stress which may be one of mechanisms of polyneuropathy by analysis of key factors for development of DPP in type 2 diabetic patients.
METHODS
Study population
The study was conducted under voluntary informed consent. Ninety patients with type 2 DM who underwent work-ups for peripheral polyneuropathy including NCV studies in Daegu Medical Center from January 2009 to November 2009. Patients were excluded from this study if they had a history of chronic alcohol consumption, hepatobiliary disorders, or any other acute disease. Those patients with blood levels greater than three times that of normal aspartate aminotransferase (AST) or alanine aminotransferase (ALT) were excluded. Patients who had neuropathy other than diabetic neuropathy, or who had problems in the evaluation of DPP due to other reasons were also excluded.
Study design and assessments
A detailed questionnaire was completed for each of the 90 participating patients. Information obtained included age, gender, smoking history, history of alcohol consumption, duration of DM, history of hypertension or cardiovascular diseases, and symptoms related to peripheral neuropathy. In addition, age, height, waist circumference, neurologic physical examination, fasting blood glucose (FBG), 2 hours postprandial blood glucose (2PPBG), C-peptide, and insulin levels were obtained. Baseline laboratory data including serum GGT, AST, ALT, glycosylated hemoglobin (HbA1c), creatinine, C-reactive protein (CRP) and lipid profiles were analyzed using the ARCHITECT c8000 (Toshiba, Tokyo, Japan).
We evaluated symptoms and the degree of DPP using the MNSI [5]. Physical examinations were performed to assess loss or weakening of the knee and ankle jerk reflexes, weakened perception to vibration, and a monofilament was used to perform tactile tests of the foot including big toes, the instep, and the sole [11].
NCV examinations were performed according to the standard method using the Synergy® instrument (Oxford Medelec, Wiesbaden, Germany) at 20 to 25℃ room temperature. The presence of polyneuropathy was documented by evaluating the latencies, amplitudes, and conduction velocities for motor nerves in both median, ulna, posterior tibial, and peroneal nerves and the latencies, amplitudes for sensory nerves in both median, ulna, sural, and superficial peroneal nerves.
There are various methods used to diagnose DPP. In the present study, DPP was defined as a positive NCV and a positive neurologic physical exam in patients with a clinical MNSI score ≥ 3 and who also had accompanying neurologic symptoms such as paresthesia, numbness, pain, and tingling sensation and there was no apparent etiology of peripheral polyneuropathy besides diabetes [12]. Diabetic retinopathy was defined as cases with proliferative retinopathy or nonproliferative retinopathy according to clinical ophthalmic examinations and the urinary albumin-creatinine ratio (ACR) was calculated to assess diabetic nephropathy [13].
Data analysis
Statistical analysis was performed using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA) and the baseline characteristics of participants were presented as the mean ± standard deviation and n (%). Data were compared using an independent-sample Student t-test for continuous data, odds ratio and Chi-square test for categorical variables, and the Mann-Whitney U test for non-parametric data with an irregular distribution. Multiple logistic regression analysis was performed to assess independent associations between key risk factors and the presence of DPP. A P value of less than 0.05 was considered statistically significant.
RESULTS
Baseline characteristics
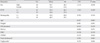
There were 46 male patients and 44 females in this study and the mean age was 59 years. The average body mass index was 24.4 (kg/m2), the waist circumference was 87.8 cm, and the waist/hip ratio was 0.9. The duration of diabetes was on average 8.7 years. The laboratory data showed a mean HbA1c of 8.0%, FBG of 8.2 mmol/L, 2PPBG of 12.9 mmol/L, C-peptide of 1.4 mmol/L, and a GGT of 42.4 IU/L. Other clinical and laboratory characteristics are listed in Table 1.
Correlation between serum GGT and clinical characteristics in subjects
The analysis for correlation of serum GGT with clinical and biochemical characteristics of the subjects indicated that gender, 2PPBG, and total cholesterol concentration were significantly associated with serum GGT level with a positive correlation (Table 2).
Clinical characteristics in type 2 diabetic patients according to the incidence of polyneuropathy
The number of patients with DPP was 36 (40%), while the number of patients without DPP was 54 (60%). The analysis of the clinical and biochemical characteristics between the two groups showed no difference in age, gender, waist circumference, duration of DM, history of hypertension, HbA1c, C-peptide, glucose levels, cholesterol concentrations, or renal function (Tables 3, 4). However, Tables 3, 4 do show that smoking history, diabetic retinopathy, systolic blood pressure (SBP), diastolic blood pressure (DBP), GGT, AST, CRP, and urine ACR in patients with DPP were significantly higher than those in patients without DPP as 50% vs. 25.9%, 77.8% vs. 51.9%, 128.9 ± 11.8 mm Hg vs. 123.1 ± 12.1 mm Hg, 80.0 ± 10.4 mm Hg vs. 76.7 ± 6.7 mm Hg, 66.1 ± 51.6 IU/L vs. 26.6 ± 15.4 IU/L, 34.1 ± 22.7 IU/L vs. 23.4 ± 10.0 IU/L, 1.3 ± 3.9 mg/dL vs. 0.9 ± 3.0 mg/dL, and 4.6 ± 8.4 µg/mg vs. 1.5 ± 3.6 µg/mg.
Multiple logistic regression model
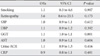
To examine the independent associations between the key risk factors and the presence of DPP, we performed a multiple logistic regression analysis with the significant eight variables - smoking, retinopathy, SBP, DBP, serum GGT, AST, CRP, and urine ACR in univariate analysis. Only increased level of serum GGT remained independently associated with the presence of DPP, which carried a relative risk with an odds ratio of 1.1 (P < 0.01) (Table 5).
DISCUSSION
Diabetic neuropathy is the most common complication of diabetes leading to foot ulcers or amputations in the future, which results in the rise in the socioeconomic burden owing to increased morbidity and mortality [3]. Hence, early diagnosis of DPP may play an important role in the prevention and treatment of foot ulcers. A number of methods have been applied for detection of DPP including the objective analysis of symptoms, neurologic physical examinations, and NCV studies. The most accurate diagnosis of DPP comprises a combination of clinical symptoms, signs, and several tests including NCV, not a single reference [14,15]. We conducted the MNSI for symptoms to detect peripheral polyneuropathy. A diagnosis of DPP required not only positive findings in NCV studies, but also supportive evidence on neurological physical examinations. Particularly, we used the MNSI score as one of standard scale for symptoms of DPP because it has been reported that a cutoff of ≥ 3 points in the continuous MNSI score was used as suggested diabetic polyneuropathy [5,12].
Oxidative stress may contribute to the pathophysiology of the onset and progression of nerve injury in diabetic neuropathy through defects in metabolic and vascular pathways [16]. Hyperglycemia increases the production of nicotinamide adenine dinucleotide (NADH). This overproduction can lead to an overload of the electron transport chain causing oxidative stress, damage to mitochondria, and activation of poly (ADP-ribose) polymerase (PARP) [16]. This activation of PARP by reactive oxygen species (ROS) induces inflammation and neuronal dysfunction in conjunction with the hexosamine and protein kinase C (PKC) pathways. The activation of advanced glycation endproducts (AGE), polyol, hexosamine, and PKC pathways with oxidative stress and hyperglycemia leads to redox imbalance, gene expression disturbance, and further oxidative stress [16]. The inflammatory and neuronal dysfunction may occur through these pathways [17]. Therefore, systemic and neural oxidative stress produced in metabolic and vascular pathways may contribute to the onset and progression of diabetic neuropathy [16]. Zotova et al. reported that single-nucleotide polymorphisms of the genes for mitochondrial and extracellular dismutases (SOD) may increase the risk for diabetic neuropathy [18]. Alpha-lipoic acid, a powerful antioxidant, regenerates the glutathione that may prevent the spread of oxidative stress. Such treatment shows a significant improvement in nerve blood flow, NCV, regeneration capacity and protection of vascular endothelial function in DPP [19,20].
It is very difficult to directly measure oxidative stress, and thus easy and inexpensive serum markers of oxidative stress are valuable. GGT has been known mainly as a marker of alcohol consumption or liver diseases, and serum GGT within normal ranges has been reported to be associated with risk factors of cardiovascular diseases and components of metabolic syndrome [21]. Although the relationship between celluar GGT and serum GGT is not clear, cellular GGT has been reported to be directly involved in the generation of ROS [22]. The inverse associations between antioxidants and serum GGT according to venous sampling analysis have indicated the possibility that serum GGT might be associated with oxidative stress [21,23]. Certain information supports this hypothesis. First, dietary heme iron has been used to positively predict the future serum GGT concentration, although the portion of free iron causing oxidative stress was not measured. Second, most dietary antioxidants such as Vitamin C, and β-carotene have been reported to predict future serum GGT concentration, in an inverse relationship. Third, serum GGT has been used to predict CRP, a marker of inflammation, and F2-isoprostanes, a marker of oxidative damage due to arachidonic acid [21]. In addition, hypertension, diabetes, and hyperlipidemia, the major risk factors of cardiovascular diseases, have been reported to be associated with oxidative stress in several recent studies [10,24,25]. In the present study, gender, postprandial blood glucose, and total cholesterol concentration were positively associated with serum GGT (Table 2). This information supports the supposition that serum GGT might be significant as a marker of oxidative stress. Therefore, we investigated whether serum GGT as a sensitive marker of oxidative stress which was considered to be part of pathophysiology of DPP might be significantly associated with the presence of polyneuropathy in type 2 diabetic patients. We found that serum GGT levels in patients with DPP were significantly higher than those in patients without polyneuropathy. Therefore we suggest that an increased level of serum GGT might have important clinical implications for the presence of DPP in patients with type 2 diabetes. In addition, smoking, retinopathy, SBP, DBP, serum AST, CRP, and urinary ACR also showed significant associations as risk factors of DPP (P < 0.05, Tables 3 and 4).
Oxidative stress is one of the key factors in metabolic syndrome including insulin resistance, hypertension, obesity, and hyperlipidemia. In metabolic syndrome, the increase in ROS induces an increased oxidative stress with over-activation of NADPH oxidase and this process may reduce the bioavailability of nitric oxide (NO), yielding low NO levels in patients with metabolic syndrome. Therefore, ROS or the increase in ROS is a key factor in metabolic syndrome, and oxidative stress is also associated with most components of metabolic syndrome [26]. Lim et al. [27] reported that serum GGT level within normal range might have an important clinical association with risk factors of cardiovascular diseases due to positive associations between serum GGT level and FBG, total cholesterol, triglyceride, and uric acid levles. Koh et al. [28] reported that age, triglyceride level, and waist circumference were important metabolic syndrome components, and that ALT and GGT levels in particular might predict metabolic syndrome. In our study, GGT and AST were significantly increased in patients with DPP. In addition, other risk factors of DPP such as age, weight, gender, duration of DM, HbA1c, glucose levels, peripheral vascular diseases, hypertension, cardiovascular diseases, and dyslipidemia have been reported [11,14,29,30]. In our study, age, gender, HbA1c, glucose levels, and lipid concentrations did not show significant associations with DPP. Particularly, smoking, hypertension, and lipid concentrations may be considered to be associated with peripheral polyneuropathy by blood flow impairment and aggravation of arteriosclerosis [11]. The current study showed that smoking, retinopathy, SBP and DBP, not lipid profiles, were significantly associated with DPP. Hypoinsulinemia, decreased insulin secretory function of the pancreas as documented by C-peptide measurements, has been reported to be an additional risk factor for the development of diabetic polyneuropathy in type 2 diabetic patients [11]. However, our study showed no significanct association with insulin secretion. Recently, it has been reported that diabetic polyneuropathy is associated with subclinical inflammation in particular with CRP, interleukin-6 (IL-6) and inversely, IL-18 [12]. CRP is an acute phase protein that is produced in the liver and induced by IL-6 mainly [12]. In our study, the CRP level measured in patients with DPP was significantly increased compared with that of patients without DPP. Other studies on the pathophysiology of DPP have been reported a decreased erythropoietin level in blood [31]. Additionally, an aldose reductase gene polymorphism [32] may play a role in the development of peripheral neuropathy in diabetic patients.
In order to examine any independent associations between the presence of DPP and key risk factors, we performed a multiple logistic regression analysis with the significant eight variables from univariate analysis. These eight factors were smoking, retinopathy, SBP, DBP, serum GGT, AST, CRP and urine ACR. It was found that only serum GGT remained significantly associated with the presence of DPP. This association was independent and carried an odds ratio of 1.1 (P < 0.01, Table 5).
There were some limitations in this study. First, only medical history and a questionnaire were used to evaluate cardiovascular events or autonomic neuropathy. The lack of clinical evaluations to detect or diagnose latent cardiovascular or autonomic complications may have caused an under-reported incidence. Recent studies have reported that cardiovascular risk factors may predict the development of large-fiber dysfunction in patients with DPP [29]. There may be a significant relationship between DPP and cardiovascular autonomic neuropathy [33]. Therefore, additional studies are necessary to evaluate this relationship. Second, strict and accurate guidelines for several tests and neurological examinations may also be necessary to avoid misleading results owing to subjective tendencies or technical variations. Third, diabetic nephropathy is usually defined by the presence of proteinuria > 0.5 g/24 hour or two out of three samples spot-collected over a 3- to 6-month period for ACR [13]. However, we investigated ACR only once on admission. Finally, there is a limit to explain the cause and pathogenesis of DPP with only oxidative stress except other factors. Future prospective long-term studies are necessary to evaluate the clinical relationship between GGT and DPP and a pathogenesis of DPP in a larger population.
In summary, this study indicates that increased levels of serum GGT may be significantly related to the presence of DPP in patients with type 2 DM. Additional studies are necessary to confirm these hypotheses to treat and prevent DPP in a larger population.



 XML Download
XML Download