

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
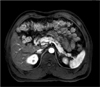
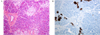
We report a 45-year-old man with type 2 diabetes who presented with recurrent hypoglycemia. Biochemical and imagingstudies did not show any mass-like lesion in the pancreas, so prednisolone and diazoxide were administered for the treatment of hypoglycemia. However, the hypoglycemia persisted during and after the medical treatment. A selective arterial calcium stimulation test was performed and revealed a suspicious lesion at the head of the pancreas. The patient underwent enucleation of the pancreas head lesion. The lesion was confirmed histologically to be focal nesidioblastosis and surgical resection was successfully performed. The patient showed no hypoglycemic symptoms postoperatively.
Figures and Tables



References
1. GF L. Nesidioblastoma, the islet tumor of the pancreas. american journal of pathology. 1938. 14:125.
2. Karnauchow PN. Nesidioblastosis in adults without insular hyperfunction. Am J Clin Pathol. 1982. 78:511–513.
3. Brown RE, Madge GE. Cystic fibrosis and nesidioblastosis. Arch Pathol. 1972. 92:53–57.
4. Brown RE, Still WJ. Nesidioblastosis and the zollinger-ellison syndrome. Am J Dig Dis. 1968. 13:656–663.
5. Bloodworth JM Jr. Morphologic changes associated with sulfonylurea therapy. Metabolism. 1963. 12:287–301.
6. Nathan DM, Axelrod L, Proppe KH, Wald R, Hirsch HJ, Martin DB. Nesidioblastosis associated with insulin-mediated hypoglycemia in an adult. Diabetes Care. 1981. 4:383–388.
7. Reinecke-Luthge A, Koschoreck F, Kloppel G. The molecular basis of persistent hyperinsulinemic hypoglycemia of infancy and its pathologic substrates. Virchows Arch. 2000. 436:1–5.
8. Fong TL, Warner NE, Kumar D. Pancreatic nesidioblastosis in adults. Diabetes Care. 1989. 12:108–114.
9. Perry RR, Vinik AI. Clinical review 72: diagnosis and management of functioning islet cell tumors. J Clin Endocrinol Metab. 1995. 80:2273–2278.
10. Yasukura K, Ono A, Woo M, Matsuzaki S, Iwase S, Kobayashi Y. A mild case of nesidioblastosis with diagnostic and therapeutic difficulty. Acta Paediatr Jpn. 1993. 35:258–261.
11. Larijani B, Aghakhani S, Lor SS, Farzaneh Z, Pajouhi M, Bastanhagh MH. Insulinoma in iran: A 20-year review. Ann Saudi Med. 2005. 25:477–480.
12. Machado MC, da Cunha JE, Jukemura J, Bacchella T, Penteado S, Abdo EE, Machado MA, Herman P, Montagnini AL, Pinotti H. Insulinoma: Diagnostic strategies and surgical treatment. A 22-year experience. Hepatogastroenterology. 2001. 48:854–858.
13. Youn JH, Joo YS, Kim BJ, Kim SH, Kwon KH, Jung MA, Yang JS, Jung IS, Kim CH, Cho SB, Lee TS, Kim EK. A case of islets cell hyperplasia diagnosed by selective arterial calcium stimulation test. J Korean Soc Endocrinol. 2001. 16:515–519.
14. Pereira PL, Roche AJ, Maier GW, Huppert PE, Dammann F, Farnsworth CT, Duda SH, Claussen CD. Insulinoma and islet cell hyperplasia: Value of the calcium intraarterial stimulation test when findings of other preoperative studies are negative. Radiology. 1998. 206:703–709.
15. Kaczirek K, Soleiman A, Schindl M, Passler C, Scheuba C, Prager G, Kaserer K, Niederle B. Nesidioblastosis in adults: A challenging cause of organic hyperinsulinism. Eur J Clin Invest. 2003. 33:488–492.
16. Jang HJ, Lee HK, Lee KU, Shong YK, Hong SK, Han DJ. Surgically correctable hyperinsulinemic hypoglycemia in adults insulinoma vs. Nesidioblastosis. J Korean Surg Soc. 1998. 55:757–768.
17. Anlauf M, Wieben D, Perren A, Sipos B, Komminoth P, Raffel A, Kruse ML, Fottner C, Knoefel WT, Mönig H, Heitz PU, Klöppel G. Persistent hyperinsulinemic hypoglycemia in 15 adults with diffuse nesidioblastosis: Diagnostic criteria, incidence, and characterization of beta-cell changes. Am J Surg Pathol. 2005. 29:524–533.
18. Goossens A, Gepts W, Saudubray JM, Bonnefont JP, Nihoul F, Heitz PU, Klöppel G. Diffuse and focal nesidioblastosis. A clinicopathological study of 24 patients with persistent neonatal hyperinsulinemic hypoglycemia. Am J Surg Pathol. 1989. 13:766–775.
 XML Download
XML Download