

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Microalbuminuria in type 2 diabetes is a predictor of development of clinical nephropathy and cardiovascular disease. But, it has been reported that reduced glomerular filtration rate (GFR) may occur in some normoalbuminuric diabetic patients. The aim of this study was to identify whether decreased GFR without microalbuminuria is to predict diabetic vascular complications.
Methods
Between January 1998 and February 2001, 73 patients with type 2 diabetes who visited Yeungnam university medical center were divided into 5 groups according to initial GFR ranges: group 1 (GFR < 30 mL/min), group 2 (30 ≤ GFR < 60 mL/min), group 3 (60 ≤ GFR < 90 mL/min), group 4 (90 ≤ GFR < 125 mL/min), group 5 (125 mL/min ≤ GFR). They were examined for microvascular and macrovascular complications initially and after 4 years.
Results
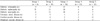
Decreased GFR had a negative correlation with age (γ = -0.472, P = 0.001). Decreased GFR without microalbuminuria had a significant correlation with development of diabetic nephropathy (P = 0.016) after 4 years. There were no significant correlation with the prevalence of diabetic retinopathy, peripheral neuropathy, and macrovacular disease. But, our study showed that coronary artery disease had an increasing tendency with decreased GFR without statistical significance (P = 0.085).
Conclusions
Our data suggest that reduced GFR, independent of albuminuria, may be an important predictor of diabetic nephropathy and coronary artery disease to some extent. So we recommend that not only the microalbuminuria, but also the decrease in GFR should be evaluated at the follow-up of patients with type 2 diabetes.
Figures and Tables
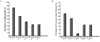 | Fig. 1A. The prevalence of diabetic nephropathy after 4 years by each group (P = 0.016). B. The prevalence of coronary heart disease after 4 years by each group (P = 0.085).
|


References
1. Knobler H, Zornitzki T, Vered S, Oettinger M, Levy R, Caspi A, Faraggi D, Livschitz S. Reduced glomerular filtration rate in asymptomatic diabetic patients. J Am Coll Cardiol. 2004. 44:2142–2148.

2. American Diabetes Association. Consensus development conference on the diagnosis of coronary heart disease in people with diabetes. Diabetes Care. 1998. 21:1551–1559.
3. Grundy SM, Garber A, Goldberg R, Havas S, Holman R, Lamendola C, Howard WJ, Savage P, Sowers J, Vega GL. Prevention conference VI: Diabetes and cardiovascular disease. Writing group IV: lifestyle and medical management of risk factors. Circulation. 2002. 105:e153–e158.
4. Dinneen SF, Gerstein HC. The association of microalbuminuria and mortality in non-insulin-dependent diabetes mellitus: a systematic overview of the literature. Arch Intern Med. 1997. 157:1413–1418.
5. Cooper ME. Pathogenesis, prevention and treatment of diabetic nephropathy. Lancet. 1998. 352:213–219.
6. Kramer HJ, Nguyen QD, Curhan G, Hsu CY. Renal insufficiency in the absence of albuminuria and retinopathy among adults with type 2 diabetes mellitus. JAMA. 2003. 289:3273–3277.
7. MacIsaac RJ, Tsalamandris C, Panagiotopoulos S, Smith TJ, McNeil KJ, Jerums G. Nonalbuminuric renal insufficiency in type 2 diabetes. Diabetes Care. 2004. 27:195–200.
8. Garg AX, Kiberd BA, Clark WF, Haynes RB, Clase CM. Albuminuria and renal insufficiency prevalence guides population screening: results from the NHANES III. Kidney Int. 2002. 61:2165–2175.
9. Henry RM, Kostense PJ, Bos G, Dekker JM, Nijpels G, Heine RJ, Bouter LM, Stehouwer CD. Mild renal insufficiency is associated with increased cardiovascular mortality: The Hoorn Study. Kidney Int. 2002. 62:1402–1407.
10. Cifkova R, Erdine S, Fagard R, Farsang C, Heagerty AM, Kiowski W, Kjeldsen S, Lüscher T, Mallion JM, Mancia G, Poulter N, Rahn KH, Rodicio JL, Ruilope LM, van Zwieten P, Waeber B, Williams B, Zanchetti A. ESH/ESC Hypertension guidelines committee: Practice guidelines for primary care physicians: 2003 ESH/ESC hypertension guidelines. J Hypertens. 2003. 21:1779–1786.
11. Atlas of end stage renal disease in the United State. USRDS 2002 Annual Data Report. 2002. Bethesda, Md: National institutes of health, National Institute of Diabetes and Digestive and Kidney Disease.
12. Xue JL, Ma JZ, Louis TA, Collins AJ. Forecast of the number of patients with end stage renal disease in the United States to the year 2010. J Am Soc Nephrol. 2001. 12:2753–2758.
13. Olson J. Jenette JC, Olson JL, Schwartz MM, Silva FG, editors. Diabetes mellitus. Hepinstall's Pathology of the Kidney. 1998. 5th ed. Philadelphia, Pa: Lippincott-Raven;1247–1286.
14. Mogensen CE, Christensen CK, Vittinghus E. The stages in diabetic renal disease. With emphasis on the stage of incipient diabetic nephropathy. Diabetes. 1983. 32:64–78.
15. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999. 130:461–470.
16. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976. 16:31–41.
17. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification and stratification. Am J Kidney Dis. 2002. 39:S1–S246.
18. Remuzzi G, Schieppati A, Ruggenenti P. Clinical practice: nephropathy in patients with type 2 diabetes. N Engl J Med. 2002. 346:1145–1151.
19. Rahman M, Brown CD, Coresh J, Davis BR, Eckfeldt JH, Kopyt N, Levey AS, Nwachuku C, Pressel S, Reisin E, Walworth C. Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial Collaborative Research Group. The prevalence of reduced glomerular filtration rate in older hypertensive patients and its association with cardiovascular disease. Arch Intern Med. 2004. 164:969–976.
20. Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, McCullough PA, Kasiske BL, Kelepouris E, Klag MJ, Parfrey P, Pfeffer M, Raij L, Spinosa DJ, Wilson PW. American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention: Kidney disease as a risk factor for development of cardiovascular disease. A statement from the American heart association councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Circulation. 2003. 108:2154–2169.
21. Sadeghi HM, Stone GW, Grines CL, Mehran R, Dixon SR, Lansky AJ, Fahy M, Cox DA, Garcia E, Tcheng JE, Griffin JJ, Stuckey TD, Turco M, Carroll JD. Impact of renal insufficiency in patients undergoing primary angioplasty for acute myocardial infarction. Circulation. 2003. 108:2769–2775.
22. Best PJ, Lennon R, Ting HH, Bell MR, Rihal CS, Holmes DR, Berger PB. The impact of renal insufficiency on clinical outcomes in patients undergoing percutaneous coronary intervention. J Am Coll Cardiol. 2002. 39:1113–1119.
23. Taniwaki H, Nishizawa Y, Kawagishi T, Ishimura E, Emoto M, Okamura T, Okuno Y, Morii H. Decrease in glomerular filtration rate in Japanese patients with type 2 diabetes is linked to atherosclerosis. Diabetes Care. 1998. 21:1848–1855.
 XML Download
XML Download