

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Chronic obstructive pulmonary disease (COPD) is a complex syndrome with significant heterogeneity, having different clinical presentation, imaging, and response to therapy1. COPD is a major cause of chronic morbidity and mortality throughout the world and its incidence is expected to increase over the coming decades2. Pneumonia is also a major cause of hospitalization and a common cause of death3. Epidemiological studies show that COPD is the most common disease associated with pneumonia4.
COPD as a risk factor for the development of pneumonia was primarily identified by studies on population-based cohorts5 or cohorts of patients with pneumonia67. It has been suggested that COPD severity is an important predictor of pneumonia hospitalization in the Unites States5. Elevations in baseline C-reactive protein levels and dyspnea index have also been suggested to be markers of pneumonia risk8. Moreover, common comorbid conditions, such as advanced age, diabetes mellitus, and cardiovascular disease, in patients with COPD may also associate with an increased risk of pneumonia. Recently, concerns is raised on that inhaled corticosteroids (ICS) use may associate with an increased incidence of pneumonia91011. Despite these reports, it is still unknown which components of COPD associate with the development of pneumonia.
Given recent advances in computed tomography (CT) technology, it may be a useful tool for evaluating the severity, extension, and distribution of the disease components of COPD at both a qualitative and a quantitative level. Indeed, recent studies have reported that particular radiological characteristics of COPD are associated with various clinical, genetic, and physiological features, such as greater lung emphysema associated with COPD exacerbations or Gly16 variant in ADRB2 gene associated with airway wall changes121314. However, it is not clear about the role of CT for predicting the development of pneumonia in patients with COPD.
It would be of interest to know which types or components of COPD are associated with the development of pneumonia because being able to predict which patients with COPD are at greatest risk of developing pneumonia may improve the understanding of the heterogeneity in COPD and facilitate better health care for these individuals. Therefore, the present retrospective study analyzed clinical features, exercise capacity, lung function, and CT measurements to identify risk factors for the development of pneumonia in patients with COPD on a prospective observational cohort.
Materials and Methods
1. Subjects
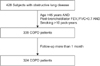
The data of 324 patients diagnosed with COPD were analyzed retrospectively. These patients were selected from the Korean obstructive lung disease (Korean OLD, KOLD) Cohort (Figure 1), which consisted of 428 stable patients with OLD who had been prospectively recruited from the pulmonary clinics of 16 hospitals in South Korea between June 2005, and February 2012. The inclusion criteria for patients with OLD have been described previously15. The patients were diagnosed with COPD if they were aged >45 years, had >10 pack-years of cigarette smoking, and had a post-bronchodilator forced expiratory volume in one second (FEV1)/forced vital capacity <0.7, but did not have bronchiectasis or sequelae of pulmonary tuberculosis. Patients who had exacerbation of COPD within the past 2 months were excluded. Patients who had been enrolled for less than 1 month were excluded because adverse events were evaluated on a monthly basis.
At the enrollment visit, all patients were evaluated with medical interviews, physical examinations, spirometry, bronchodilator reversibility tests, and lung volume, and 6-minute walk tests. Health-related quality of life was evaluated by calculating the total score of St. George's Respiratory Questionnaire (SGRQ). Comorbidity scores were calculated by using an updated Charlson comorbidity index16. Chronic bronchitis was defined by a questionnaire that identified the patients who had a chronic cough and phlegm production for 3 months per year for at least 2 consecutive years. In addition, volumetric CT was performed to evaluate airway wall thickness, emphysema severity, and mean lung density (MLD) ratio at full expiration and inspiration at the enrollment visit.
Our Institutional Review Board approved the analyses of the clinical and imaging data (Institutional Review Board of Asan Medical Center, 2012-0484). Individual informed written consent was obtained from all patients.
2. Pulmonary function tests
The method for pulmonary function tests have been described previously15. Spirometry was performed by using a Vmax 22 (Sensor-Medics, Yorba Linda, CA, USA) or a PFDX (MedGraphics, St. Paul, MN, USA). To assess post-bronchodilator FEV1 increases, spirometry was performed before bronchodilation and 15 minutes after inhalation of salbutamol 400 µg through a metered-dose inhaler with a spacer. Bronchodilator reversibility was evaluated by measuring post-bronchodilator FEV1 increase in liters. Lung volumes were measured by body plethysmography (V6200; Sensor-Medics or PFDX). Diffusing capacity for carbon monoxide (DLco) was measured by the single-breath method using a Vmax229D (Sensor-Medics) or a Masterlab Body (Jaeger AB, Würtsburg, Germany). All pulmonary function tests were performed as recommended by the American Thoracic Society (ATS)/European Respiratory Society (ERS).
3. Computed tomography
Volumetric CT scans were obtained by using a 16-multidetector CT scanner (Somatom Sensation Instrument; Siemens, Erlangen, Germany; GE Lightspeed Ultra instrument; General Electric Healthcare, Milwaukee, WI, USA; Philips Brilliance instrument; Philips Medical Systems, Best, The Netherlands) as previously described17. The volume fraction (%) of the lung below -950 Hounsfield units (HU) at full inspiration was calculated automatically (Inspiratory V950) from the CT data. The ratio of MLD on expiration and inspiration was calculated. The airway dimensions, wall area (WA), lumen area (LA), and wall area percent [WA%; i.e., WA/(WA+LA)×100] were measured near the origin of two segmental bronchi (the right apical and left apico-posterior) that were selected by consensus by two radiologists. Emphysema index as Inspiratory V950, air trapping index as MLD ratio, and airway thickening as WA% were significantly correlated with clinical parameters in patients with COPD17.
4. Pneumonia definition
No definition of pneumonia existed in the KOLD study protocol. Therefore, episodes of pneumonia were identified from the adverse events that were reported at unscheduled visits and at regular visits every 3 months. In this study, a pulmonary physician reviewed the clinical and radiological information of all respiratory adverse events, retrospectively. The event of pneumonia was selected among the record if the attending physician had treated for pneumonia, and the reviewing physician agreed with diagnosis of pneumonia on the basis of respiratory symptoms, laboratory finding, and pulmonary infiltration on chest radiography. Only episodes of community-acquired pneumonia were included in this study. Three episodes of healthcare-associated or nosocomial pneumoniawere identified and all were excluded from the analysis in this study.
5. Statistical analysis
To investigate risk factors associated with the development of pneumonia, Cox proportional hazard analysis was used for univariate and multivariate analyses. Censoring occurred at the date of the first episode of pneumonia, the date of dropout, and the date of death reported on death certificate or the date when the participant was last known to be alive. Selected potentially independent variables were age, sex, body mass index (BMI), total SGRQ score, Charlson comorbidity score, symptom of chronic bronchitis, 6-minute walking distance (6MWD), current smoking status, smoking pack-years, post-bronchodilator FEV1 (% of predicted), bronchodilator reversibility (FEV1 changes in liter), 3-month treatment response of FEV1 (L), and CT measurements (V950, WA%, and MLD ratio). Multicollinearity was assessed using variation index factor for analyzing multivariate factors. Kaplan-Meier plots were generated to show the development of pneumonia over time in patient groups that were categorized according to the severity of emphysema. Additionally, the patients were classified into three groups on the basis of emphysema extent, as indicated by the CT measurement of inspiratory volume fraction (%) of the lung below –950 HU (V950). The patients in the 33th percentile or less, the 34th to 66th percentile, and the 67th percentile or greater were catagorized as having mild, moderate, and severe emphysema, respectively.
The SAS version 9.2 (SAS Institute Inc., Cary, NC, USA), and SPSS version 15 (SPSS Inc., Chicago, IL, USA) were used for data analysis, with p-values <0.05 considered to be significant.
Results
The mean age of the patients with COPD was 66.7±7.5 (mean±standard deviation) years, the mean smoking amount was 47.5±26.9 pack-years, and the mean post-bronchodilator FEV1 was 53.8±16% of predicted values. Men made up 97% of the patients. Of the 324 patients with COPD, 28 (8.6%) developed pneumonia. The median follow-up time for all patients was 1,099 days (range, 40–2,428 days) and the median time to the development of pneumonia was 772 days (70–2,172 days) (Table 1).
The unadjusted Cox proportional hazard analyses showed that age, BMI, SGRQ, 6MWD, post-bronchodilator FEV1, and the CT measurements V950 and MLD ratio associated with the development of pneumonia in the patients with COPD (Table 2). Multivariate Cox proportional hazard analysis showed that only post-bronchodilator FEV1 and the CT measurements of emphysema extent were independent risk factors (Table 3).
The subjects were classified into three groups on the basis of the magnitude of CT measurements of emphysema extent. The patients in the 33th percentile or less were categorized as having mild emphysema (CT emphysema extent [mean±standard deviation], 7.4±4%); those in the 34th to 66th percentile were categorized as having moderate emphysema (21.4±4.7%); and those in 67th percentile or greater were categorized as having severe emphysema (42.6±7.6%). Figure 2 shows that the patients with severe emphysema were more likely to develop pneumonia over time (log-rank [Mantel-Cox] test, p<0.001).
Discussion
This study showed that the extent of emphysema, as evaluated by CT imaging, and airflow obstruction of FEV1, as measured by spirometry, were independent risk factors for the subsequent development of pneumonia by patients with COPD during a median follow-up period of 3 years. It also suggested that the extent of emphysema associated more strongly with the subsequent development of pneumonia than other physiological measurements in patients with COPD. On this basis, the extent of emphysema, as evaluated by CT imaging, seems to be important for evaluating the condition of patients with COPD.
A population-based study reported that pneumonia risk associates with older age, male gender, comorbid conditions, smoking status, and the degree of lung function impairment5. In addition, COPD itself is the underlying disease that is most frequently associated with pneumonia4. Moreover, in the Towards a Revolution in COPD Health (TORCH) study, two of the ICS-containing arms associated with increased incidences of pneumonia, with the combination arm exhibiting a doubling of the incidence from 4% to 8% over the 3-year period9, while some studies argue that ICS may be in fact protective of severe pneumonia and improve mortality18. The present study showed that age, male gender, smoking status, comorbid conditions, and the use of ICSs were statistically not independent risk factors for pneumonia in COPD, although it should be noted that the statistical power of the study may have been low: only 28 of the 324 patients developed pneumonia. Moreover, the statistical significance may have been low for some variables because comorbid conditions occurred infrequently in our COPD cohort and because most patients had been treated with ICSs. Moreover, smoking status after enrollment could have changed because most patients were advised to stop smoking and the patients who entered the cohort were thought to have good compliance. However, with respect to the study's focus upon which types or components of heterogeneous COPD associate with the development of pneumonia, the clinical significance of the study may be increased if the effect of other factors, such as comorbid conditions, use of ICSs, and smoking status were mitigated.
Recently, it was reported that the airflow limitation grade and the presence of pulmonary emphysema were independently associated with the development of severe pneumonia in a Korean COPD population admitting a hospital19. It is consistent that the present study also showed an independent risk factors of the airflow limitation, FEV1, and an emphysema in development of pneumonia. Meanwhile, it is known that the presence of emphysema on CT scan does not indicate a severe COPD, emphysema is a phenotype of COPD. We analyzed emphysema extent quantitatively, and showed the extent of emphysema associated with the subsequent development of pneumonia.
CT has become an increasingly important tool for evaluating smoking-related lung disease. Quantitative measurements of COPD by CT include emphysema severity, airway wall thickness, and air trapping. Increasing emphysema severity, as defined by CT, associates with poor health status20 and increased mortality21. Recently, greater lung emphysema severity and airway wall thickness, as measured by CT, were found to associate with COPD exacerbations13. The present study showed that of the CT measurements, only emphysema extent associated with pneumonia. Patients with COPD present with anatomo-pathological changes in the bronchial mucosa that facilitate colonization of the lung by potentially pathological microorganisms, which may lead to episodes of pneumonia or COPD exacerbation. However, it is unclear how each phenotype, as defined by CT, relates to the development of pneumonia and the exacerbation of COPD. On the other hand, our findings did show that chronic bronchitis did not associate with the development of pneumonia, whereas it had been previously reported that the chronic bronchitis phenotype in patients with COPD associated with a higher risk of exacerbations22. It is also unclear how each clinical phenotype related to the development of pneumonia and the exacerbation of COPD. If the association between possible etiological factors, such as airway inflammation or emphysema, and COPD exacerbation or pneumonia is clarified, our understanding of COPD heterogeneity and pathophysiology will improve. It seems apparent that the role of CT scan is advancing in patients with COPD. In practice, however, more evidences are required to perform CT scan on all patients, considering effectiveness and adverse effects of CT such as radiation exposure, availability and cost.
Our study showed that the development of pneumonia became more common over time in the group of patients with severe emphysema. In addition, the three emphysema groups differed significantly in terms of their initial treatment responses (3-month FEV1 change after combined treatment with long-acting beta2 agonist and ICS): as the emphysema severity increased, the less increase in FEV1 after treatment was observed. The mean FEV1 increase was 178±237 mL in the mild emphysema group, 135±293 mL in the moderate emphysema group, and 62±185 mL in the severe emphysema group (Table 4). The poor treatment response of the patients with severe emphysema suggests that there should be caution regarding the use of ICSs in these patients, as these drugs may only serve to increase the pneumonia risk. Large randomized control trials examining both the risks and benefits of ICSs may be needed to help direct the proper use of ICSs in patients with emphysema.
The present study also had other limitations. First, the retrospective nature of this study may have hampered the accurate identification of episodes of pneumonia. This reflects the fact that a definition of pneumonia did not exist in the study protocol. It is possible that unreported pneumonia existed. It is also possible that patients may have been misdiagnosed with a COPD exacerbation when it was actually pneumonia, or vice versa. However, every event in all patients was reviewed closely. Moreover, the incidence of pneumonia in patients who were treated with ICSs was similar to that found in other studies 1011. Second, our study subjects were predominantly male smokers, probably due to the very low prevalence of female smokers in Korea. Further investigations are warranted for identifying gender differences of pneumonia risk in patients with COPD. Third, there was little information in the present study regarding the severity of the pneumonia episodes, the pathogenic microorganisms that were involved, the pneumococcal vaccination status of the patients, and the appropriateness of the therapy the patients received for the infection. The characteristics of pneumonia that occur in patients with COPD warrant more research. Fourth, the influence on the patient's dose (i.e., medium vs. high) of ICS and the compliance to the medication regimen were not investigated. It remains a controversial topic and further research is required.
In conclusion, this study showed that emphysema severity measured by CT and post bronchodilator FEV1 are important risk factors for the development of pneumonia in COPD.





 XML Download
XML Download