

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Scrub typhus is an acute febrile illness caused by Orientia tsutsugamushi. It is endemic to the 'tsutsugamushi triangle,' which areas of South East Asia, the Indian subcontinent, Sri Lanka, Indian Ocean islands, Papua New Guinea, and North Queensland12. It is characterized by fever, headache, mental confusion, a macular rash, and an eschar. The majority of patients can recover with early diagnosis and proper management.
But, in spite of the availability of treatment such as doxycycline, scrub typhus with severe complication is still regarded as a fatal disease. As previous reports345, the mortality rate of scrub typhus ranges from 16.7% to 30% in Southeast Asia. Severe complications can be manifested by acute respiratory distress syndrome, encephalitis, interstitial pneumonia, myocarditis, acute renal failure, and acute hepatic failure6. In case of accompanying acute respiratory failure, the patients have to admit to intensive care unit (ICU) and should be treated with mechanical ventilation. The prognostic risk factors for mechanical ventilation in those patients may provide a timely initiation of appropriate therapy, reduce a respiratory arrest and the mortality rate of scrub typhus.
To our knowledge, there has been few study on the risk factors for mechanical ventilation in patients with scrub typhus. Therefore, we conducted this study to evaluate the risk factors for mechanical ventilation in the patients with scrub typhus admitted to ICU at a university hospital for the last 10 years.
Materials and Methods
1. Study population and data collection
We retrospectively analyzed data of 70 patients who were consecutively admitted to ICU of Eulji Universivy Hospital, Daejeon, Republic of Korea and diagnosed with scrub typhus between May 2004 and December 2014. The diagnosis of scrub typhus was based on the World Health Organization's criteria7. When an immunofluorescent antibody assay (IFA) titer against O. tsutsugamushi increased more than four times or an indirect IFA IgM titer against O. tsutsugamushi to ≥1:80, scrub typhus was confirmed.
The following data were collected from medical records: age, gender, vital signs, months at admission, reasons for ICU admission, comorbidities, symptoms, and laboratory findings at admission, transfusion, inotropic agent, eschar, death, cause of death, total duration of hospitalization, duration of ICU stay, Acute Physiology and Chronic Health Evaluation (APACHE) II score, and Sequential Organ Failure Assessment (SOFA) score.
2. Definitions
In this study, we divided study patients into the following two groups: the mechanical ventilation group (MV group) and the non-mechanical ventilation group (non-MV group). We considered mechanical ventilation if patients were treated with mechanical ventilation, whether the time of diagnosis was before or after mechanical ventilation. Sepsis was defined by the present of both infection and systemic inflammatory response syndrome (SIRS). SIRS was considered if patients fullfilled at least two of the following criteria: body temperature <36℃ or >38℃, heart rate >90 beats per minute, respiratory rate >20 breaths per minute, leukocyte count <4,000 or >12,000 cells/µL or the presence of more than 10% band forms. Neurologic problem was defined by the presence of central nervous system (CNS) related symptoms such as confusion, seizure, or coma. Acute respiratory failure was defined not only by the result that hypoxemia, hypercapnia, or both cannot be maintained within normal ranges, but also by the presence of symptoms and signs resulted in the need for mechanical ventilation, pneumonia, pleural effusion, pulmonary edema, or acute respiratory distress syndrome. Cardiac problem was defined by the presence of symptoms and signs result in pericardial effusion, ischemic heart failure, and arrhythmia such as atrial fibrillation, ventricular tachycardia, and complete atrioventicular block. Acute renal failure was defined as at least 50% reduction in glomerular filtration rate using the abbreviated modified diet in renal disease equation.
3. Statistical analysis
Continuous variables were compared using the two-tailed Student's t test. Categorical data were analyzed using the chi-square test. Factors associated with mechanical ventilation were analyzed by binary linear regression models. Univariate binary logistic regression analysis was done. Then, multivariate analysis was done with the significant factors in the univariate analysis. Results were reported as mean±standard deviation or number (%). Data was collected in Microsoft EXCEL (Microsoft Excel 2007; Microsoft Corp., Seattle, WA, USA) and all statistical analysis were performed using SPSS version 14.0 (SPSS Inc., Chicago, IL, USA). All p-values were 2-tailed and statistical significance was considered when p-value was less than 0.05.
Results
1. Clinical features of the patients with scrub typhus admitted to ICU
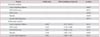
A total of 70 patients, 32 (45.7%) were males, 15 (21.4%) had rash, 35 (50.0%) had eschar, and seven (10%) were dead. The mean age of patients was 71.2±11.1 years (Table 1). The antibiotic treatment between 69 patients and one non-mechanical ventilation patient were doxycycline and flumoxef plus clarithromycin, respectively. The most common reasons of the patients admitted to ICU were acute respiratory failure in MV group and sepsis in non-MV group. Statistically significant differences were observed in acute respiratory failure between the two groups (p=0.008). Clinical features were analyzed between MV group and non-MV group (Table 1). The mean of peak airway pressure, positive end-expiratory pressure, fraction of inspired oxygen (FiO2), and tidal volume in MV group were 14.6±3.2 mm Hg, 5.6±3.8 mm Hg, 71.6±21.2%, and 437.4±68.7 mL, respectively. There were statistically significant differences in APACHE II score (p=0.015), and death (p=0.014) between two groups. In comparison of laboratory features between two groups, there was no statistically significant difference (Table 2).
2. Factors associated with mechanical ventilation in the patients with scrub typhus admitted to ICU
We analyzed factors associated with mechanical ventilation in the patients with scrub typhus admitted to ICU. In univariate analysis, acute respiratory failure at admission to ICU (p=0.005), APACHE II score (p=0.017), SOFA score (p=0.020), platelet count (p=0.058), and lactate dehydrogenase (LDH) (p=0.074) were statistically significant factors (Table 3). In multivariate analysis, acute respiratory failure at admission to ICU (odds ratio [OR], 6.289; 95% confidence interval [CI], 1.517-26.071; p=0.011), SOFA score (OR, 1.453; 95% CI, 1.119- 1.888; p=0.005), APACHE II score (OR, 1.187; 95% CI, 1.040- 1.353; p=0.011), platelet count (OR, 1.010; 95% CI, 1.002-1.017; p=0.009), and LDH (OR, 1.002; 95% CI, 1.000-1.003; p=0.011) were independent significant factors associated with mechanical ventilation in the patients with scrub typhus admitted to ICU (Table 3).
3. Various periods and chronological orders of the patients with scrub typhus admitted to ICU between mechanical ventilation and non-mechanical ventilation
We analyzed various periods of the patients with scrub typhus between MV group and non-MV group. There was statistically significant differences in the duration of ICU stay between two groups (p=0.028). However, there were no statistically significant differences in the duration of hospitalization, and doxycycline treatment before admitting to ICU between two groups (Table 4).
Discussion
In this study, the mortality rate of patients with scrub typhus admitted to ICU was 10.0%. As previous reports performed in ICU345, the mortality rate of scrub typhus ranges from 16.7% to 30% in Southeast Asia. The mortality rate of ICU in our study was lower than that of previous reports345; however, the reason was not understood exactly. We found that the patients with mechanical ventilation represented 27.1% of all patients with scrub typhus admitted to ICU. Acute respiratory failure was the most common reason of ICU admission in MV group (47.4%). The mortality rate of MV group and non-MV group were 26.3% and 3.9%, respectively. The results of the present study revealed that the factors leading patients with scrub typhus to mechanical ventilation were acute respiratory failure, SOFA score, APACHE II score, platelet count, and LDH. By logistic regression analysis, they were defined as significant variables associated with mechanical ventilation.
There were a few reports of clinical features, laboratory findings, and risk factors leading to fatal outcome associated with severe scrub typhus2689. However, to our knowledge, there was few report of risk factors leading to mechanical ventilation in patients with scrub typhus admitted to ICU.
Previous studies2689 have reported that the risk factors for severe scrub typhus were age ≥60 years, CNS dysfunction, white blood cell (WBC) counts >10,000/µL, total bilirubin >2 mg/dL, albumin ≤3.0 g/dL, creatinine ≥2 mg/dL, APACHE II score, and SOFA score. In our study, the population, patients with scrub typhus admitted to ICU, fulfilled the results of previous studies as showing that age was 71.2±11.1 years, WBC counts was 12,600/µL, and albumin was 3.0±0.5 g/dL. But, the parameters of CNS dysfunction, total bilirubin, and creatinine were different from previous studies (Tables 1, 2)2689.
In multivariate analysis, the parameters which can be the meaningful indicators of mechanical ventilation for the patients with scrub typhus admitted to the ICU were SOFA score (p=0.005), platelet count (p=0.009), acute respiratory failure (p=0.011), LDH (p=0.011), and APACHE II score (p=0.011).
It was surprising to find that LDH was significantly associated with mechanical ventilation for patients with scrub typhus admitted to ICU by multivariate analysis. LDH has been one of medical significant indicators, because it is extensively found in body tissues, such as heart muscle and blood cells. Because it is released during tissue damage, it can be a marker of injuries and disease. Ogawa et al.10 reported that elevated levels of LDH was observed in 91%. Tachibana et al.11 reported that severe type scrub typhus seemed to have the higher mean value of LDH. Venkategowda et al.12 reported that increase LDH was statistically significant (p<0.0001) in scrub typhus patients group with acute respiratory distress syndrome. In our study, the mean levels of LDH were 1,516.2 IU/L in MV group, and 863.1 IU/L in non-MV group (Table 2). So, the levels of LDH can be the one of meaningful indicators of mechanical ventilation for the patients with scrub typhus admitted to ICU.
The association between acute respiratory failure and mechanical ventilation are not surprising. The patients with scrub typhus admitted to ICU should be carefully monitored, and the intensivists should prepare to mechanical ventilation, if they initially had complication of acute respiratory failure.
Griffith et al.8 reported that APACHE II scores were significantly higher (p=0.007) in patients with scrub typhus who needed invasive mechanical ventilation (21.32±8.6) when compared with those requiring non-invasive ventilation (16.63±7.24). In our study, it is different from point of view that we compared APACHE II scores between MV group and non- MV group (p=0.015).
There was statistically significant differences in the duration of ICU stay between MV group and non-MV group in our study (p=0.028) (Table 4). However, in case of MV group, the duration of ICU stay included the duration of mechanical ventilation. So, when the duration of only non-mechanical ventilation between two groups was analyzed, we found that significant differences were not observed (p=0.782).
There are few limitations in this study. First, our study was retrospectively designed from a single medical center, such as the bias in selection of patient or mechanical ventilation. So, the results of our study may not be extrapolated as general. Second, specific circumstance of our institution and geographic distribution of O. tsutsugamushi might affect clinical feature, laboratory, and treatment of scrub typhus. Third, we could not analyze the difference in virulence according to genotypes of O. tsutsugamushi. As previous report13, genotypes may be related to the virulence of scrub typhus in patients with scrub typhus admitted to ICU. So, we thought that the genotypes would be one of risk factors to increase the admission of ICU, acute respiratory failure, and mechanical ventilation. Therefore, prospectively designed, a large number of patients, and multi-center studies should be performed to overcome these limitations.
In conclusion, we found that acute respiratory failure, SOFA score, APACHE II score, platelet count, and LDH can be the meaningful indicators of mechanical ventilation for the patients with scrub typhus admitted to ICU.



 XML Download
XML Download