

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cough is one of the most common symptom of many respiratory diseases. Although cough guidelines from various countries are available, there has been no Korean cough guideline. The Korean Academy of Tuberculosis and Respiratory Diseases organized cough guideline committee at March 2013. From March 2013 to October 2014, cough guideline was developed by the members of this committee. The purpose of this guideline is to help clinicians to diagnose correctly and treat efficiently patients with cough. The content of this guideline is confined to adult patients only. This guideline is developed based on evidence. The committee developed key questions and searched evidence in three medical databases, Medline, Embase, Cochrane library and also in three Korean journals, Tuberculosis and Respiratory Diseases, Korean Journal of Medicine, and Allergy, Asthma & Respiratory Disease. The level of evidence was evaluated by the Grading of Recommendations Assessment, Development and Evaluation approach1. The strength of recommendation was assigned by formal voting rules from expert committee. The Korean cough guideline is written in Korean and published October 2014. In this article, we have stated recommendation and summary of Korean cough guideline.
3. Acute and subacute cough
1) Recommendation
- Beta-2 agonist should not be used to improved cough symptom (evidence, low; recommendation, strong).
- Considering adverse effect of antibiotics, empirical therapy of antibiotics can be considered only in patients with purulent sputum (evidence, high; recommendation, weak).
2) Summary
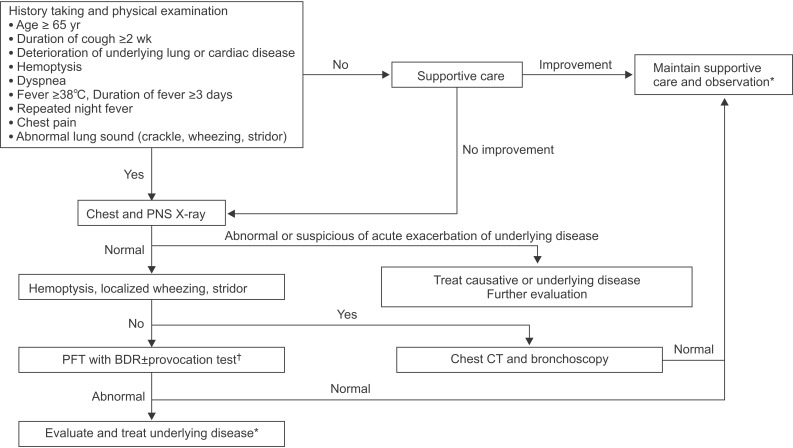
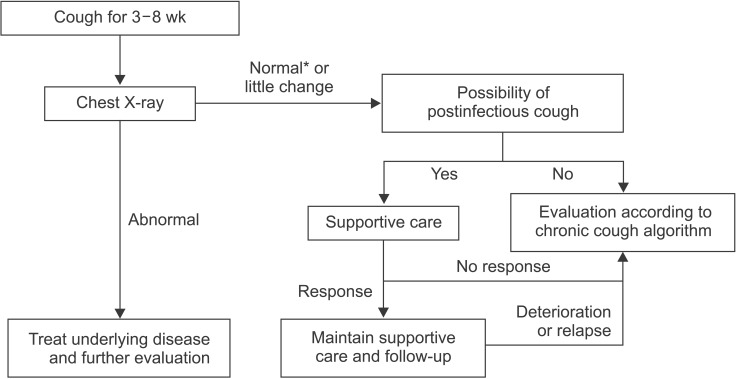
- Acute cough can be early symptom of serious diseases such as acute exacerbation of interstitial lung disease (ILD), congestive heart failure, tuberculosis (TB), endobronchial neoplasm, or foreign body aspiration. Thus, these diseases should be included in the differential diagnosis of acute cough (Figures 1, 2).
- Considering prevalence of TB in Korea, chest X-ray should be checked in patients with acute cough whose duration is more than 2 weeks.
- Chest X-ray can be checked in acute cough patients with old age, since symptoms of serious diseases may be non-specific in them.
4. Chronic cough
1) Summary
- Chronic cough is defined as a cough lasting more than 8 weeks.
- History including smoking, accompanying symptom, and medication is helpful for differential diagnosis and should be taken first and enough.
- Test for upper airway cough syndrome (UACS), cough variant asthma (CVA), and gastroesophageal reflux disease (GERD) should be performed (Figure 3).
5. Upper airway cough syndrome
1) Recommendation
- In UACS, intranasal steroid can be considered in order to improve cough (evidence, very low; recommendation, weak).
- In UACS, oral anti-histamine is recommended to improve cough (evidence, very low; recommendation, strong).
- In UACS, using nasal decongestant only is not recommended to improve cough (evidence, expert opinion; recommendation, strong).
- In UACS, intranasal anti-histamine is not considered to improve cough (evidence, very low; recommendation, weak).
- In UACS, antibiotics is not recommended to improve cough (evidence, expert opinion; recommendation, strong).
2) Summary
- UACS is syndrome of which various upper airway disease cause cough.
- UACS is diagnosed based on symptom, physical examination, radiologic finding, and response to empirical treatment.
- If UACS is diagnosed, adequate treatment should be initiated.
- If UACS is suspicious, first generation anti-histamine and nasal decongestant can be used empirically.
6. Cough variant asthma
7. Eosinophilic bronchitis
8. Gastroesophageal reflux disease
9. Chronic bronchitis
1) Recommendation
- In chronic bronchitis (CB) with normal lung function, smoking cessation is recommended in order to improve cough (evidence, expert opinion; recommendation, strong).
- In CB with normal lung function, mucoactive agent can be considered in order to improve cough (evidence, expert opinion; recommendation, weak).
2) Summary
- Treatment for CB with decreased lung function should follow chronic obstructive pulmonary disease guideline.
- CB is the most common cause of cough in smokers.
- Mucoactive agent is effective on improvement of cough in CB with decreased lung function22.
10. Bronchiectasis
1) Summary
- When bronchiectasis is suspicious, high resolution computed tomography (HRCT) is needed even if chest X-ray is normal26.
11. Bronchiolitis
1) Recommendation
- In diffuse panbronchiolitis, low-dose macrolide antibiotic is recommended in order to improve cough (evidence, expert opinion; recommendation, strong).
2) Summary
- Bronchiolitis should be preferentially considered when there are irreversible airflow obstruction, suspicion of small airway disease in HRCT, and purulent sputum in patients with cough31.
12. Lung cancer
1) Summary
- Chest X-ray should be performed in case of risk factor for lung cancer or metastatic lung cancer.
- Bronchoscopy should be performed when suspicious of endobronchial invasion by tumor even if chest X-ray is normal32.
- In lung cancer, the reason of cough may not come from cancer. Thus, further evaluation is needed.
- In lung cancer, cough should be managed actively since it can affect quality of life and prognosis33.
- In lung cancer, stepwise treatment based on mechanism of drug should be considered in order to control cough34.
13. Aspiration
1) Summary
- Oropharyngeal dysphagia and aspiration should be checked in case of cough being developed when eating or swallowing food35.
14. Angiotensin converting enzyme inhibitor
15. Habit, psychogenic cough
1) Summary
- Habit, psychogenic cough is unconsciously persistent cough without underlying disease. It can be considered when there is no obvious reason for cough or cough does not respond to conventional therapy38.
- Habit, psychogenic cough is developed mostly during pediatrics and adolescent. When developed in adult, it may accompany with psychological problem3940.
- Habit, psychogenic cough is characterized by aggravation during emotional stress and social activity and disappearance during sleep.
- Habit, psychogenic cough can be diagnosed only if other causes are ruled out38.
17. Cough due to environmental and occupational factor
1) Summary
- Environmental and occupational factors can evoke cough in itself, or can aggravate cough due to other causes. Thus, consideration for environmental and occupational factors is mandatory.
- Detailed history taking of exposure and occupation is important to find environmental and occupational factors.
23. Idiopathic cough
24. Treatment agent of cough: antitussive and mucoactive agent
1) Summary
- Narcotic central antitussive: morphine, codeine
- Nonopioid central antitussive: dextromethorphan, levopropoxyphene
- Peripheral antitussive: benzonatate, benproperine, theobromine
- Etc.: amitriptyline, baclofen, gabapentin
Mucoactive agent can be classified as expectorants, mucoregulatory agents, mucolytics, and mucokinetics5354
- Expectorants: hypertonic saline, iodinated glycerol, domiodol, guaifenesin, ion channel modifiers
- Mucoregulatory agents: carbocysteine, anticholinergics, glucocorticoid, macrolide antibiotics
- Mucolytics
- Mucokinetics: inhaled SABA, methylxanthine, surfactant, ambroxol, acebrophylline

 XML Download
XML Download