

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In 2009, the American Joint Committee on Cancer (AJCC) and the Union Internationale Contre le Cancer (UICC) published the seventh edition of the TNM Classification of Malignant Tumors, which was introduced for use in clinical practice from January 1, 2010. The seventh edition of the classification system applies to non-small cell lung cancer (NSCLC), small-cell lung cancer (SCLC)1 and bronchopulmonary carcinoids23. The lymph node map proposed by the International Association for the Study of Lung Cancer (IASLC) was incorporated into the new TNM staging for lung cancer4.
Prior to the publication of the seventh edition, some discrepancies existed in lymph node nomenclature between the two lymph node maps most widely used in clinical practice, the Japanese (Naruke)5 and the Mountain-Dressler modification of the American Thoracic Society map (MD-ATS)6. The most significant difference between these relates to the description of subcarinal lymph node. The new IASLC lymph node map attempted to reconcile the differences between these two lymph node maps and to provide more precise anatomic definitions for all lymph node stations4. This internationally agreed uniform classification system is crucial for treatment planning, for assessing treatment outcomes, and for optimizing future analyses of the prospective international database currently being collected, to facilitate evidence based adjustments for the upcoming eighth edition of the UICC and AJCC staging manuals due to be completed in 2016.
Currently, computed tomography (CT) and positron emission tomography-CT are used routinely for clinical staging of lung cancer, CT having the advantage of greater special resolution and availability. The aim of this article is to review the anatomical definitions of the IASLC lymph node map and provide practical illustration of the mapping system on CT. Moreover, we will give a detailed account of the important changes incorporated in the seventh edition, which affect tumor staging. This simplified illustration of the nodal map provides a useful tool for use in day-to-day clinical practice not only for radiologists but also oncologists, surgeons and pathologists who are involved with the staging and management of patients with lung carcinoma.
Classification of the Lymph Node Staging (N) in the IASLC Map
The N classification labels the extent of lymph node metastases. The N staging is unchanged on the IASLC map compared with the sixth edition with the N staging validated by survival analysis. The nodal groups by N stage are as follows: N1, ipsilateral intrapulmonary, peribronchial and hilar; N2, ipsilateral mediastinal and subcarinal; and N3, contralateral mediastinal or hilar nodes, ipsilateral or contralateral supraclavicular nodes7. Positive nodes outside the above-defined regions are classified as distant metastasis (M1b).
CT Anatomy of Lymph Node Stations
The anatomic descriptions of each lymph node station have been more precisely described to avoid any overlap in definition between stations. In the IASLC map, the number of lymph node stations is the same as that of sixth edition. However, the 14 stations are reorganized from four groups into seven zones. This new grouping is based on retrospective survival analyses of international databases and lays the foundation for future prospective database centered survival analyses8910.
1. Supraclavicular zone: station 1
In the MD-ATS map, the supraclavicular zone lymph nodes were classified as superior mediastinal nodes. However, in the IASLC map station 1 nodes are considered extrathoracic lymph node and all station 1 lymph nodes are classified as N3 disease.
2. Upper zone: station 2R, 2L, 3a, 3p, 4R, and 4L
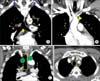
The location descriptions and anatomic boundaries of station 2, 3, and 4 are shown in Table 2 and Figures 2 and 3.
The upper border of stations 2, and 3 is the apex of the lung and pleural space, and in the midline, the upper border of the manubrium. The lower borders of stations 3, 4R, and 4L differ from each other (Figure 2A, B). The lower border of 2R serves as the upper border of 4R, and the same applies for the border between 2L and 4L. For both station 2 and 4, the border between 2R and 2L and between 4R and 4L moves from the midline of the trachea to the left lateral border of the trachea in the IASLC map. This is one of the major changes made in N mapping in the seventh edition (Figure 2C, D).
In the IASLC map definition, the lower border of station 1 is the clavicle bilaterally and, in the midline, the upper border of the manubrium and the upper border of station 2 and 3 extends higher up to the lung apex than the lower border of station 1. Therefore, on axial image, the posterior border of station 1 can abut the anterior border of station 2 or 3p (Figure 4). Because the definitions of the lower border of station 1 nodes are not identical to the definition of the upper border of station 2 and 3 nodes and because the position of the clavicles can vary depending on the level of arm elevation, the inferior-lateral border of station 1 nodes may vary leading to overlap between these nodal groups. The lymph nodes that are closer to the midline are hardly ever affected by the position of the arms11. It would be helpful if the definition of the lower border of station 1 and the upper border of station 2 were identical. This is an improvement, which might be considered for the eighth edition.
3. AP zone: stations 5 and 6
The location descriptions and anatomic boundaries of station 5 and 6 are listed in Table 3.
The medial border of station 5 is the ligamentum arteriosum (Figure 5), which is difficult to identify on axial CT unless calcified. The prevalence of ligamentum arteriosum calcification on CT is higher in children (37.8%) than in adults (11.2%) with peak prevalence in 6-10 years, afterwards declining with age12. Although usually invisible on CT the expected location can be estimated by identifying the closest position of the upper pulmonary artery and the aortic arch on coronal reconstructions.
Station 6 lymph nodes lie anterior and lateral to the ascending aorta and aortic arch (Figure 6). The anterior border of station 6 is the imaginary horizontal line extending from the anterior wall of the aortic arch (Figure 6B). In radiological staging it is not clinically important to differentiate stations 5 and 6, both of which lie in the aorto-pulmonary nodal region and differentiation does not affect staging.
4. Subcarinal zone: station 7
The location description and anatomic boundary of station 7 is listed in Table 4.
Station 7 encompasses a larger area in the new seventh edition IASLC map than on previous map versions and is most easily identified on the coronal images (Figure 7A). This is one of the major changes and reconciles the Naruke and MD-ATS maps11.
The nodes located in the space between the medial margins of both main bronchi are station 7 and nodes outside of the space are station 10 (Figure 7B)413. Below the carina of the trachea, the nodes in the posterior mediastinum are station 7 and above this level 3p. Within the cranio-caudal boundary of the subcarinal zone, the posterior margin of station 7 extends posteriorly to the paraesophageal area at this level (Figure 7B) with station 8 upper boundary below this level. Station 7 nodes are considered ipsilateral (N2) with the primary tumor irrespective of side.
5. Lower zone: station 8 and 9
The location descriptions and anatomic boundaries of station 8 and 9 are listed in Table 5.
Below the lower border of subcarinal zone, station 8 nodes lay adjacent to the wall of the esophagus and to the right or left of the midline (Figure 8).
Station 9 nodes are located within the inferior pulmonary ligament (Figure 9) and separation of station 8 and 9 is easy at surgery. In the region of the inferior pulmonary vein, the mediastinal and visceral pleura merge to form the inferior pulmonary ligament. It extends downwards toward to the hemidiaphragm anchoring the lower lobes to the mediastinum. The length of this ligament may vary both from person to person and in the same individual1415.
6. Hilar/interlobar zone: station 10 and 11
The location descriptions and anatomic boundary of station 10 and 11 are listed in Tables 6 and 7, respectively.
Station 10 includes the nodes immediately adjacent to the mainstem bronchus and hilar vessels such as the proximal portions of the pulmonary veins and main pulmonary arteries. There is a change of the borders between station 4 and 10 with the pleural reflection no longer serving as the border between them (Figure 10)4. The lymph nodes around the both main bronchi within the mediastinum are considered as station 10; the nodes below the lower margin of the azygos vein as 10R, and the nodes below the upper rim of the left main pulmonary artery as 10L. Therefore, some tumors previously staged as N2 are now staged as N1. Pitson et al.16 and El-Sharief et al.17 discussed a potential ambiguity for lymph nodes at the level of the tracheal bifurcation below the level of the superior vena cava-azygos vein junction, and grouped lymph nodes anterior to the tracheal bifurcation with the lower paratracheal station17. However, Lee et al.18 reported that the changed definition between N1 and N2 diseases by IASLC map works well in classifying patient prognosis.
Station 10 also has a common boundary with station 7 and border is a vertical line from the medial margin of the both main bronchi (Figure 7B).
7. Peripheral zone: station 12, 13, and 14
Station 12 is a node adjacent to the lobar bronchi. Station 13 is a node adjacent to the segmental bronchi. Station 14 is a node adjacent to the subsegmental bronchi. These nodes are intrapulmonary and for staging purposes are to be differentiated from intrapulmonary metastasis. Differentiation affects staging as an intrapulmonary metastasis in the same lobe as the primary tumour would be a T3 cancer while station 12, 13, or 14 nodes would be N1 disease. Nodes are usually peribronchovasular often at areas of bronchial branching.
Future Analyses for the Next Edition
The seventh edition IASLC map was formulated after retrospective analysis of outcome data for a multinational database. The seventh edition IASLC map therefore provided more precise anatomic definitions than that of sixth edition, however there remain several outstanding areas of uncertainty, which could be addressed, in later editions.
(1) There is no specific definition of the border between right and left side for station 3a, 3p, and 8, which is necessary to classify N2 or N3 tumour. It is unclear whether this should be the midline or the left side of the trachea as when categorising station 2 and 4 nodes.
(2) Some lymph nodes in the thorax, which lung cancer only occasionally metastasises to, are not included in the IASLC lymph node map at all. These include anterior, middle, and posterior diaphragmatic nodes, intercostal nodes, internal mammary node, retrocrural nodes and axillary node. It is unclear whether these should be classed as N2 or N3 disease.
(3) The IASLC classification doesn't relate the relationship between overall survival and lymph node burden addressing issues such as single metastases versus multiple metastases, the significance of skip metastases and extranodal tumour spread.
Uniform application of the IASLC map will provide the database for future prospective analysis to solve the ambiguities and to make more complete lymph node classification.
Summary
The seventh TNM staging and IASLC map are applied to NSCLC, SCLC, and bronchopulmonary carcinoids.
The major changes in the IASLC nodal map are as follows: (1) border between station 2R and 2L moves from the midline of trachea to the left lateral wall of the trachea (Figure 2C, D); (2) border between station 4R and 4L moves from the midline of trachea to the left lateral wall of the trachea (Figure 2C, D); (3) station 7 encompasses a larger area in the IASLC map and this reflects reconciliation between the Naruke and MD-ATS maps (Figure 7); (4) there is a change of the borders between station 4 and 10 with the pleural reflection no longer serving as the border between the two stations (Figure 10).

















 XML Download
XML Download