

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Bronchial anthracofibrosis (BAF) is characterized by definite narrowing or obliteration of large airways with anthracotic pigmentation in the bronchial mucosa1. Although anthracotic pigmentation is caused primarily by the inhalation and deposition of carbon particles along with iron, lead, cadmium and other organic or inorganic materials2, BAF is generally not associated with pneumoconiosis or smoking1. According to a few recent studies, it has shown a close association with exposure to wood smoke, as a result of burning fuels for cooking and heating, particularly in poorly ventilated spaces1,3. Consequently, BAF develops mostly in elderly women1,3,4. The original diagnosis of BAF is made when multiple dark pigmentations are observed on the bronchial mucosa on bronchoscopy2,3. On computed tomography (CT) scan, BAF is characterized by multiple lobar or segmental bronchial wall thickening and narrowing combined with surrounding lymph node enlargement with or without atelectasis1,3,4,5.
BAF is frequently associated with tuberculosis, pneumonia, lung cancer, and chronic obstructive pulmonary disease (COPD)2,3. In pulmonary function testing (PFT), patients with BAF commonly exhibit obstructive ventilatory impairment2,3. Data from recent meta-analyses consistently demonstrated that biomass smoke, including wood smoke exposure, is a risk factor for COPD6,7,8. Therefore, there is a possibility that patients with BAF could be diagnosed as COPD alone, if not undergoing further evaluation for BAF. In South Korea, BAF is frequently recognized in clinical practice, and several studies regarding BAF in Korean patients have been published1,3,4,5. We hypothesized that a proportion of patients with COPD exacerbation might have BAF, not just COPD in Korea. The aim of the present study was to investigate the prevalence of BAF in patients with COPD exacerbation and to examine the clinical features of these patients.
Materials and Methods
1. Patients
Between August 2008 and April, 2012, a cohort of COPD exacerbation hospitalized to the Kyungpook National University Hospital (KNUH), a tertiary referral center (Daegu, Korea) were analyzed retrospectively. This study was approved by the Institutional Review Board of the KNUH, which waived the requirement for written informed consent because of the retrospective nature of the study. According to the criteria of the Global Initiative for Chronic Obstructive Lung Diseases9, COPD was diagnosed on the basis of the available spirometric data. COPD exacerbation was defined as acute deterioration from a stable state requiring hospitalization10. On arrival at the hospital, evaluation of patients was performed by emergency or internal medicine department physicians through history taking, physical examination, chest radiographs, and routine laboratory tests. Patients with any specific causes identified on these examinations, including pneumonia, pneumothorax, and congestive heart failure, were excluded. After exclusion, all patients underwent chest CT scan with or without contrast enhancement within 24 hours of admission to the hospital. Based on CT findings, cases with other causes which could result in lymph node enlargement, such as lung cancer and interstitial lung diseases, were also excluded. The etiology of COPD exacerbations was determined as follows: 1) pneumonia was diagnosed when consolidation or focal ground-glass opacity (GGO) was observed on CT scan; 2) tracheobronchitis if symptoms suggestive of respiratory infection, including increased sputum, purulent sputum, fever, or symptoms of upper respiratory infection (sore throat or rhinorrhea with myalgia) were identified without consolidation or focal GGO on CT scan or if centrilobular nodule or a tree-in-bud pattern suggestive of bronchiolitis was observed on CT imaging without consolidation or GGO; 3) congestive heart failure, when CT findings suggestive of pulmonary edema and echocardiographic left ventricular dysfunction coexisted11; 4) similar to an earlier study12, pulmonary embolism on CT scan as a sharply delineated pulmonary arterial filling defect present in at least two consecutive image sections and located centrally within the vessel or with acute angles at its interface with the vessel wall; and 5) undetermined, when the etiology could not be determined.
The diagnosis of BAF was based on the CT findings that fulfilled the following criteria: 1) bronchostenosis that caused smooth narrowing of multiple lobar or segmental bronchi; 2) calcified or non-calcified lymph node enlargement adjacent to narrowed bronchi; and 3) these two criteria which could not be attributed to other causes (Figure 1)4,5. All patients were classified into patients with BAF (BAF group) and without BAF (non-BAF group) according to the presence or absence of CT findings consistent with BAF. A variety of clinical variables and CT findings were compared between the two groups.
2. Clinical data
Demographic and clinical variables of the patients were checked, including gender, age, smoking history, body mass index, and comorbid conditions. History of exposure to wood smoke and its duration was retrospectively taken by an interviewer over the phone. For severity of illness, BAP-65 classes were assessed13. BAP-65 score was defined as follows: class I, patients≤65 years of age without any three risk factors (blood urea nitrogen level≥25 mg/dL, altered mental status, or pulse≥109 beats/min); class II, patients>65 years of age with no risk factors; and class III, IV, and V, patients with one, two, and three risk factors, respectively. With respect to clinical course, hospital stay and treatment outcome (improvement, transfer, or death) were recorded.
PFT data were obtained according to the standards of the American Thoracic Society and European Respiratory Society Guideline14. Spirometric data within six months before and after index admission date for comparison of airflow obstruction between the BAF and non-BAF groups were used in statistical analysis. Laboratory data included white blood cell (WBC) count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), procalcitonin, N-terminal-pro-B-type natriuretic peptide (NT-proBNP), troponin I, D-dimer, and arterial blood gas analysis data.
3. Radiologic data
CT scans were reviewed by two radiologists and a consensus diagnosis was reached. In addition to the presence of BAF, we checked for the presence of consolidation, GGO, bronchiolitis, emphysema, bronchiectasis, bronchial wall thickening, pleural effusion, and inactive pulmonary tuberculosis. These CT findings were defined as follows: consolidation as airspace opacification with obscuration of the underlying vasculature15; GGO as less densely increased attenuation without obscuration of the underlying vasculature15; bronchiolitis as centrilobular nodules with either V- or Y-shaped branching linear opacities16; emphysema characterized by the presence of areas of abnormally low attenuation near the center of the secondary pulmonary lobule or diffuse areas of low attenuation with little intervening normal lung17; bronchiectasis when the internal diameter of the bronchus was greater than that of the adjacent pulmonary artery (PA); and inactive pulmonary tuberculosis when irregular lines and calcified nodules along with distortion of bronchovascular bundles were located in upper lobes and superior segments of lower lobes18. The presence of bronchial wall thickening was considered when radiologists initially suspected the presence of bronchiectasis at 5th or 6th generation bronchi but then, on comparing the caliber of the bronchus to the adjacent artery, determined that there was no bronchial dilatation19. Thus, the bronchus looked more prominent than normal without features of bronchiectasis.
To determine the prevalence of pulmonary hypertension, we measured main PA size and PA-to-ascending aorta (AA) ratio. Similar to previous studies20,21, we measured the diameters of PA and AA at the level of the PA bifurcation in order to obtain PA size and PA-to-AA ratio (Figure 2). The widest short axis diameter of the PA and the diameter of AA in its longest diameter were measured using computer calipers. As in previous studies, PA size>33 mm21 and PA-to-AA ratio>122 were selected as the cutoff values for pulmonary hypertension.
4. Echocardiography
Transthoracic echocardiographic findings, including right ventricular (RV) dysfunction and RV systolic pressure (RVSP), were also reviewed. RV dysfunction was defined as RV free wall hypokinesia, and RVSPs were calculated using tricuspid regurgitation flow velocity as determined by Doppler echocardiography23. RVSP>40 mm Hg was selected as the cutoff value for pulmonary hypertension.
5. Statistical analysis
SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) was used in performance of statistical analyses. The data are expressed as the mean±standard deviation or median with interquartile range (IQR), if the data were skewed for continuous variables and number with percentage for categorical variables. Kappa statistic was used for measurement of the agreement between bronchoscopy and CT in determining the presence of BAF. Between the two groups, continuous variables were compared using the Student's t-test or the Mann-Whitney U test, whereas categorical variables were compared using either chi-squared test or Fisher's exact test.
Results
1. Demographic and clinical characteristics
Blinded to bronchoscopic finding, radiologists determined the presence or absence of BAF based on CT findings in 30 patients for whom both bronchoscopic results and CT images were available. Kappa statistic for diagnosing was 0.933 between bronchoscopy and CT. Initially, 209 patients were included in this study but three were excluded due to stage III or IV lung cancer (n=2) or pneumoconiosis (n=1). Consequently, a total of 206 patients were included in the final analysis and 51 (25%) were diagnosed as having BAF based on CT scan.
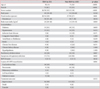
Patients with BAF were significantly older (78±7.6 years vs. 71±9.8 years, p<0.001) with female preponderance (61% vs. 23%, p<0.001) (Table 1). The BAF group included more never-smokers than the non-BAF group (52% vs. 18%, p<0.001). As expected, history of exposure to wood smoke was significantly more common in the BAF group, compared to the non-BAF group (59% vs. 27%, p=0.001). Symptoms suggestive of respiratory infection were observed less frequently in the BAF group than the non-BAF group (73% vs. 90%, p=0.001). No difference in BAP-65 class was observed between the two groups. In addition, no significant differences in length of hospital stay and treatment outcome were observed between the two groups.
Respiratory tract infection, including tracheobronchitis and pneumonia, was the most common cause of COPD exacerbation in both groups, however, its frequency was significantly lower in the BAF group, compared with the non-BAF group (77% vs. 90%, p=0.011) (Table 1). Conversely, patients with unknown cause were more common in the BAF group, compared with the non-BAF group (18% vs. 7%, p=0.017).
2. Laboratory and spirometric data
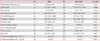
Peripheral blood WBC count and blood levels of ESR, CRP, procalcitonin, troponin-I, and D-dimer did not differ significantly between the two groups (Table 2). However, significantly higher serum level of NT-proBNP was observed, compared with the non-BAF group (425 pg/mL [IQR, 133-1,666 pg/mL] vs. 207 pg/mL [IQR, 93-755 pg/mL], p=0.018). Postbronchodilator values of percent predicted forced expiratory volume in 1 second (FEV1) and FEV1/forced vital capacity were significantly higher in the BAF group, compared with the non-BAF group (78±28.3% vs. 59±24.3%, p<0.001; and 54±13.6% vs. 43±13.7%, p=0.001, respectively), suggesting that patients with BAF had less severe airflow obstruction than those without BAF.
3. Computed tomographic and echocardiographic findings
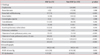
Of various CT findings, frequencies of emphysema and bronchial wall thickening were significantly greater in the non-BAF group, compared with the BAF group (80% vs. 33%, p<0.001; and 92% vs. 73%, p<0.001, respectively) (Table 3). The frequencies of the remaining CT findings did not differ between the two groups. Both PA size and PA-to-AA ratio were significantly greater in the BAF group, compared with the non-BAF group (35±5.5 vs. 31±5.0, p<0.001; and 0.95±0.15 vs. 0.85±0.13, p<0.001, respectively). The frequencies of patients with PA size>33 mm and PA-to-AA ratio >1 were significantly higher in the BAF group, compared with the non-BAF group (59% vs. 28%, p<0.001; and 43% vs. 11%, p<0.001).
Echocardiographic pulmonary hypertension was frequently observed in the BAF group, as compared with the non-BAF group (50% [6/12] vs. 18% [6/33], p=0.033), although echocardiographic data were available in the minority of the patients.
Discussion
In the current study, approximately 25% of Korean patients with COPD exacerbation had CT findings consistent with BAF. The current data demonstrated that in Korea, BAF is common in nonsmoking elderly women and that among patients presenting with COPD exacerbation, the severity of illness and clinical course are similar regardless of BAF. Of note, patients with BAF had milder airflow limitation, compared to those without BAF. However, signs of pulmonary hypertension were more common with a more severe grade in the BAF group, compared with the non-BAF group.
In developing countries, such as Mexico and Columbia, where biomass fuel has been used for heating and cooking in poorly ventilated spaces, a considerable number of patients with obstructive airway disease, particularly in nonsmoking elderly females, are caused by exposure to wood smoke3,24,25. Nowadays, biomass smoke is considered an independent risk factor for COPD6,7. In the current study, BAF was suspected in a quarter of patients presenting with COPD exacerbation. Patients with BAF who do not undergo bronchoscopy or chest CT scan can be diagnosed as having only COPD. Symptoms suggestive of respiratory infection were noted less frequently in the BAF group, compared with the non-BAF group. Thus, patients with unknown causes of COPD exacerbation were more common in the BAF group. One explanation is that BAF was found in older patients, who were less likely to recognize their respiratory symptoms. However, the possibility of other undetected causes of COPD exacerbation could not be excluded.
Patients with BAF had less severe airflow limitation, compared to those without BAF. This finding corresponds to the previous report24. This could not be exactly explained. On CT scan, BAF is characterized by stenosis of larger airways and less frequent peripheral bronchial wall thickening, compared to non-BAF COPD. In contrast, emphysema was observed less frequently in the BAF group. This finding concurred with that of a previous study showing that pathologically, emphysema was more severe in the cigarette smoke-induced COPD group, compared to the biomass smoke group26. In addition, patients with BAF can exhibit a mixed restrictive-obstructive pattern in addition to obstructive defect3. These findings suggest that the disease entity of BAF may be different from that of non-BAF COPD.
It is noteworthy that the BAF group more frequently had signs of pulmonary hypertension and more severe degree of pulmonary hypertension than the non-BAF group. This is in an agreement with a necropsy finding where intimal thickening was more severe in the biomass smoke-induced COPD group, compared with the cigarette smoke-induced COPD group26. As more fibrosis is microscopically observed in the lung parenchyma as well as in the walls of the airways of COPD patients exposed to biomass smoke26, fibrosis of the lung parenchyma can promote the occurrence of pulmonary hypertension. However, evidence of lung parenchymal fibrosis was not observed on CT of the BAF group in the present study. We speculate that extrinsic compression of pulmonary arteries by adjacent peribronchial fibrosis of larger airways may contribute to more common and severe pulmonary hypertension in patients with BAF like fibrosing mediastinitis27. However, this finding was not noted on CT of the BAF group.
Whether BAF is a phenotype of COPD or a distinct entity remains to be clarified. Biomass smoke, such as wood smoke, is considered a risk factor for COPD. However, BAF is thought be one end of the spectrum of wood smoke-induced lung diseases28. BAF is characterized by radiologically bronchial narrowing and thickening of larger airways, physiologically less severe airflow limitation, and hemodynamically more severe and common pulmonary hypertension, suggesting that the pathogenesis of BAF may differ from that of tobacco smoke-related COPD which results from a mixture of small airway disease and parenchymal destruction.
Several limitations of the current study should be considered. First, although bronchoscopy is needed to confirm BAF, the diagnosis was based on CT findings in this study. However, the CT findings of BAF are well-established, and agreement rate between bronchoscopy and CT scan in diagnosis of BAF was high for 30 patients whose bronchoscopic data were available. Second, as this study was retrospective, some clinical data were not available. Thus, selection bias could not be avoided. Third, history of exposure to wood smoke and its duration was taken by an interviewer over the phone. Recall bias should be considered. Finally, as our criteria for tracheobronchitis and pneumonia were broad, there is a possibility that the frequencies were overestimated.
In conclusion, BAF should be considered in Korean patients with presenting with COPD exacerbation, particularly in nonsmoking elderly females with a history of exposure to wood smoke. Compared with non-BAF COPD, BAF is characterized by less frequent emphysema and bronchial wall thickening on CT scan, less severe airflow limitation, and more common pulmonary hypertension with a greater degree of severity. From these results, BAF is a distinct phenotype of obstructive lung disease.


 XML Download
XML Download