

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Pulmonary systemic arterialization to the normal basal lung without sequestration is a rare congenital anomaly. In this rare abnormality, arterialization of left lower lobe is the most common type. The involved lung has normal bronchial distribution, that does not include true sequestration.
In general, surgical treatments have been performed, and recently, the embolization has been attempted.
We report the case of a 22-year-old man who was being presented with recurrent hemoptysis due to large systemic arterializations on basal segment of the right lower lobe of the lung, without sequestration. A therapeutic transarterial embolization using vascular plug was successfully performed. After embolization, he suffered from post-embolization syndromes such as pulmonary infarction with pneumonia. After 2 weeks of antibiotics therapy, he was discharged when the pneumonia improved. For the following 28 months, there have not been any hemoptysis and other complications. Our case represent that large pulmonary anomalous systemic artery can be treated by transarterial embolization when using vascular plug.
Case Report
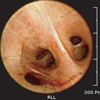
A 22-year-old man was being referred to our hospital due to hemoptysis. He experienced hemoptysis 16 months ago. The non-contrast outside chest computed tomography (CT) missed the anomaly thereafter. Otherwise, his past medical history and family history were not remarkable. Physical and laboratory findings were within normal limits. A chest radiograph demonstrated no active lung lesions. Chest CT with contrast enhancement showed a ground-glass attenuation and consolidation in the right lower lobe posterior basal segment and a large anomalous artery from the distal descending thoracic aorta supplying basal segment of right lower lobe (Figure 1). The diameter of the feeding artery was about 10 mm. Bronchoscopy revealed that the major bronchial branches were normal and at the right 2nd carina there were bleeding evidences and woozing on saline washing (Figure 2). Angiography showed about 10 mm diameter feeding artery to basal segment of right lower lobe, enlarged arteriovenous vessels and draining vein. On diagnosis of anomalous systemic arterial supply to the basal segments of right lower lobe from descending aorta without sequestration, the therapeutic embolization was performed with Amplatzer Vascular Plug (two 12 mm; AGA Medical, Golden Valley, MN, USA) (Figure 3).
After the embolization, the patient suffered from fever. At 2 days after embolization, chest X-ray revealed hazy and nodular opacities at right lower lobe (RLL). With a suspected diagnosis of post-embolization syndrome with pneumonia, the patient was prescribed to empirical antibiotics. Although the fever subsided 5 days later, his chest X-ray showed pleural effusion in the right lung (Figure 4). A diagnostic thoracentesis revealed amber colored fluids, which was found to be neutrophil-predominant exudates. At 14 days after the antibiotics application, he was discharged when symptoms and conditions had improved, but pleural effusion sustained. Twenty-two days later, his chest CT revealed vascular plugs, anomalous systemic artery from distal descending aorta, together with decreased size of subsegment veins, posterior subpleural consolidation, RLL that seemed pulmonary infarction and mild right pleural effusion. After 1 month of follow-up, chest X-ray indicated no lung lesions.
He recovered well after embolization for 2-year follow-up without complications (Figure 5).
Discussion
Anomalous systemic arterial supply to normal segments of the lung is a rare congenital anomaly. Anomalous systemic arterializations of right lower lobe is even more rare. Some authors mentioned this anomaly within the spectrum of pulmonary sequestration such as Pryce et al. classification1,2. Although it is included in the Pryce type 1 according to the original classification of pulmonary sequestration, it differs from the normal connection of the bronchial tree3.
The etiology of a systemic arterial supply to normal lung is unknown, the most likely theory is a persistent embryonic connection between aorta and pulmonary parenchyma due to failures of regression from the primitive aortic branches to the developing lung bud4.
The basal segments of left lower lobe are the most commonly affected sites, although there are other sites which can be rarely affected. The systemic artery usually varies from the thoracic aorta, but can also arise from abdominal aorta or celiac axis, and very rarely from the left subclavian and internal mammary artery5,6. These vessels usually enter the lung at the level of pulmonary hilum or at the level of inferior pulmonary ligaments. The venous drainage is normal and is accomplished by inferior pulmonary vein draining into the left atrium3.
Most patients are asymptomatic. The most common symptom is recurrent or massive hemoptysis during adulthood5. This is related to the higher pressure of systemic circulations as compared to pulmonary circulations. Other manifestations include exertional dyspnea, murmur in the lower chest and congestive heart failure due to left heart overload3. Chest radiographs often show ill-defined opacity corresponding to the anomalous artery7. Therefore, incidentally, a chest radiographs for health screening has often found the anomaly. CT angiography can demonstrate the origin and course of aberrant artery.
Treatment is recommended to symptomatic patients but also to asymptomatic patients owing to the risks of hemorrhagic complications8.
The classic therapeutic approach is surgical resection. In recent years, because of high surgery related morbidity and mortality, (vascular plug 8-AV malformation) the endovascular embolization technique has been increasingly used for the treatment of this disease. Mainly, the endovascular materials used coils5,9,10,11. However, in this case, the diameter of the feeding artery was about 10 mm which could be associated with high risks of incomplete occlusion, recanalization and embolization of the coil12.
The Amplatzer Vascular Plug is a self-expandable cylindrical mesh device which is intended for the treatment of atrial septal defect and patent ductus arteriosus. Since being described, there have been sporadic case reports on its use in the literature. Vessels occluded with the device include aortopulmonary collaterals, pulmonary arteriovenous fistulas, venovenous collaterals, shunts, coronary fistulas, and certain types of patent ductus arteriosus13.
The Amplatzer Vascular Plug is particularly suited for the embolization of large and high-flow vessels where coil migration is possible or where multiple coils may be needed12,14. In our case, large pulmonary anomalous systemic artery of basal segment of the right lower lobe of the lung, without the sequestration presenting recurrent hemoptysis can be treated by transarterial embolization when using vascular plug. Although he suffered from post embolization syndromes and complications after the embolization for 2 weeks, he had no complications for 2 years of follow-up. Our case present that large pulmonary anomalous systemic artery can be treated by transarterial embolization when using the vascular plug.




 XML Download
XML Download