

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
High-dose-rate endobronchial brachytherapy (HDREB) alone or with external beam radiotherapy is used in the treatment of endobronchial lung cancer for the main purpose of symptom relief1,2. In addition to, it can bring local treatment and life prolongation in inoperable cases of early endobronchial cancer3-5.
However, HDREB can cause massive hemoptysis in 7~32% of patients, which is a serious complication of brachytherapy1,6-8. Most of investigators explained the pathogenesis of hemoptysis is due to cancer progression or recurrence2,7. But, a recent study reported about complication of HDREB in localized and early endobronchial cancer and showed the result that fatal hemoptysis after HDREB was a complication of the treatment itself5.
According to several reports about outcome of HDREB in Korea, occurrence of fatal hemoptysis has been reported as about 2.5% to 16%9,10. However, in all of them, the purpose of HDREB was to relieve symptom in advanced lung cancer which was previously treated with surgery or external beam radiation therapy.
Therefore, we report a case of patient with massive hemoptysis who was diagnosed radiation bronchitis after HDREB for localized endobronchial squamous cell carcinoma.
Case Report
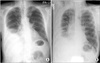
A 67-year-old man visited for cough and sputum lasting for 5 months. He was a current smoker with a history of 40 pack-year smoking and had a coronary arterial disease. Right pleural effusion was seen in a chest X-ray (Figure 1). The character of pleural effusion was exudates with many lymphocytes and low level of adenosine deaminase. A consolidation was seen in computed tomography (CT) after the effusion had been drained (Figure 2A) and no endobronchial lesion was found on left upper lobe in chest CT (Figure 2B). Bronchoscopy was performed to differentiate causes of the right lung lesion. There was no endobronchial lesion in right bronchial tree. Incidentally, mucosal nodularity was observed in the left upper lobe bronchus (Figure 3A) and was diagnosed with squamous cell carcinoma with biopsy (Figure 3B). A pulmonary wedge resection and pleural biopsy were performed to evaluate right lower lobe and pleural lesions through video assisted thoracoscopic surgery, and the results were chronic organizing pneumonia and subpleural fibrosis with chronic inflammation. The lesions of right lower lobe and right pleura were remained without progression until the last follow-up radiologic examination. Lymph node involvement and distant metastasis were not observed in the staging work-up. Despite the clinical stage was IA, the patient had moderate chronic obstructive pulmonary disease (post-bronchodilator forced expiratory volume in 1 second, 1.74 L) and his endobronchial cancer involved the left main bronchus. The patient might be intolerable for surgical treatment, such as pneumonectomy or sleeve lobectomy, and we decided to do curative local therapy.
HDREB was performed with 6 fractions of 5 Gy for 6 weeks. After the treatment, the patient complained of persistent cough, but bronchoscopy and chest CT had not shown the progression of lung cancer until 4 weeks after HDREB. Further follow-up bronchoscopies were performed at 34, 50, 54, and 59 weeks after the HDREB. Grade 1 radiation bronchitis was observed in the left upper lobe bronchus which was previous cancer lesion at 34 weeks (Figure 4A) and was also observed in the medial wall of the left mainstem bronchus which was not cancer lesion but contact area of guide sheath for radiation source at 50 weeks after HDREB (Figure 4D). On the bronchoscopic finding at 54 weeks (12 months), mucosal necrosis of the left upper lobe bronchus was advanced (Figure 4B) and ulcer lesions began to appear in the left main bronchus (Figure 4E). The patient started taking oral steroids at 55 weeks, but the area of the left upper bronchial lesions extended (Figure 4C) and left main bronchus ulcers also increased in the depth and extent at 59 weeks (14 months) (Figure 4F). Bronchial biopsies for the bronchitis were performed four times among five follow-up bronchoscopic examinations, and it showed acute or chronic inflammation and no cancer cells were observed. The patient died suddenly due to massive hemoptysis at 15 months after HDREB.
Discussion
HDREB have been undergone for the purpose of curative treatment for early lung cancer as well as the relief of symptoms of advanced lung cancer, which is obtaining a positive result and is becoming increasingly performed. When HDREB is applied to patients with localized endobronchial cancer, it is usually performed using a protocol of 6 fractions of 5 Gy at intervals of one week. The two-year locoregional control rate is 60% to 85% and two-year overall survival rate is 47% to 78% in localized early lung cancer3-5. However, this treatment approach can lead to massive hemoptysis, which leads to high mortality1,6-8.
Speiser and Spratling11 categorized bronchial inflammation and stenosis that occurs after HDREB into four grades and defined them radiation bronchitis. According to their classification, Grade 1 consists of a slight inflammation with swelling and thin whitish membrane. Grade 2 consists of an increase in white fibrous membrane with great exudation. Grade 3 consists of a severe inflammatory response with a marked membranous exudate. The final progression, Grade 4 bronchitis is greater fibrosis with resulting circumferential stenosis. The mean time to developing Grade I and IV lesions were 16 weeks and 55 weeks. Taulelle et al.12 divided radiation bronchitis into 5 grades. Grade 5 consists of bronchial wall necrosis which cause fistula formation. They explained that late fistula formation is the ultimate phase of radiation bronchitis, while early fistulae are results of massive tumor shrinkage. Interestingly there were two separated ulcerations in this case. One was at the targeted cancer lesion of left upper lobe, and the other was developed on the medial wall of left mainstem bronchus. We supposed the ulceration of left mainstem bronchus was developed by radiation effect during in and out of radiation source on the area that contacted guide sheath for radiation source. On the bronchoscopic findings of this case swelling and exudates as the Grade 1 to 3 of radiation bronchitis were the early changes, and then it progressed to necrosis and ulcer about one year after brachytherapy. We have assumed that fistula developed after last bronchoscopy and was followed by massive hemoptysis.
The mortality due to hemoptysis after HDREB for treatment of early endobronchial cancer is 0% to 4.4%3-5. Even if it is less frequent than in case of palliative HDREB, predicting occurrence of hemoptysis, preventing and treatment of hemoptysis are crucial.
The risk factors of massive hemoptysis after HDREB are radiation dose2,8, laser treatment underwent in the same region6,8, repeated brachytherapy in the same region2,8, treatment for palliative aim2,7, endobronchial tumor size7, developing radiation bronchitis11, local treatment failure and contact of brachytherapy applicator with the bronchial wall that close to major blood vessels6. Hennequin et al.7 reported a patient who died from massive hemoptysis after HDREB for lung cancer in right upper lobe bronchus and suggested a relationship between the location of the cancer and occurrence of massive hemoptysis. Hara et al.6 reported that massive hemoptysis occurs frequently in patients whose used applicator touched directly bronchial wall facing the major blood vessels in CT. In the post-mortem examination in 2 patients, fistula formations were identified between superior vena cava and trachea in one case and between left pulmonary artery and left main bronchus in another case. But, in this study, all patients with massive hemoptysis failed to control cancer by local treatment, so it is unclear which is more involved to occurrence of massive hemoptysis either local failure or relationship with major blood vessels. In our case, no treatment but HDREB was performed for cancer treatment and there was no recurrence after macroscopic and microscopic remission. According to the previous reports, only risk factor expected in this patient was the location of the cancer lesion including some of the left upper lobe bronchus that was close to left pulmonary artery, the one of the major blood vessels. And it suggests the possibility of fistula formation between the bronchial lumen and left pulmonary artery due to radiation bronchitis.
Hemoptysis can be developed by other treatment modalities for inoperable early endobronchial cancer. Incidences of hemoptysis are 7.8% in photodynamic therapy13, and 4% in cryotherapy14. But, there is no investigation about direct comparison of the treatment modalities.
Since HDREB-treated patients experiencing massive hemoptysis cannot usually be managed by any special methods and most of them cannot survive, which is the fatal weakness of HDREB. In our case, despite the patient has taken steroids, prescribed frequently in radiation pneumonitis, depth and width of necrosis and ulceration had been worse in follow-up bronchoscopy. Matsumoto et al.15 proposed the surgery as a way to treat ongoing bronchial necrosis. They performed omentum wrapping around left main bronchus via laparoscopic and open thoracotomy for a treatment of progressive ulcer. And the bronchial ulcers became a little worse after the surgery, it has shown an improvement with normal mucosa. In addition, they mentioned that bronchial artery embolization for endobronchial necrosis and hemoptysis is not effective because they failed to treat hemoptysis occurred after HDREB and experienced the patient's death. In our case, bronchial lesions progressed from small range of radiation bronchitis to deep necrosis which caused massive hemoptysis without microscopic recurrence of cancer. That suggests massive hemoptysis could be occurred after HDREB as a direct complication of the treatment regardless of local control. The only symptom that we predict endobronchial change was persistent cough. But there was no symptom that can predict massive hemoptysis. In addition, radiologic imaging of the treated area remained unchanged. Eventually, follow-up bronchoscopy is the only diagnostic modality to predict fatal hemoptysis especially in patients with upper lobe bronchus lesions which show proximity to the major blood vessels. The median time of the onset of massive hemoptysis after HDREB is approximately 3~12 months1,2,4,5,7,8,10. During the periods, patients should be monitored stringently. Once radiation bronchitis is observed, physicians should keep in mind the lesion may progress to ulceration and massive hemoptysis may occur. However, specific treatment for radiation bronchitis and HDREB related hemoptysis has not been established, the more investigation for development of medical or surgical treatment will be needed.



 XML Download
XML Download