

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Acute pulmonary embolism (PE) ranges from asymptomatic to often fatal, incidentally discovered emboli to massive embolism causing immediate death. Acute PE may occur rapidly and unpredictably and may be difficult to diagnose. Mortality and complications can be reduced by prompt diagnosis and therapy. Untreated PE is associated with a mortality rate of approximately 30 percents. Most patients with PE have endogenous fibrinolysis, although it is not effective enough to prevent PE. A case of spontaneous remission of untreated acute PE has not previously been reported. Here we present a case of spontaneously resolved acute PE without any treatment.
Figures and Tables
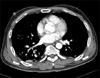
Figure 1
Chest AP on ER shows multiple patch consolidations in right lung. AP: anteroposterior; ER: emergency room.

References
1. Park YS, Ha JW, Kwon KH, Jang YS, Chung NS, Shim WH, et al. Clinical characteristics and predictors of in-hospital mortality for patients with acute major pulmonary embolism. Korean J Med. 2000. 58:293–300.
2. Tapson VF. Acute pulmonary embolism. N Engl J Med. 2008. 358:1037–1052.
3. Carson JL, Kelley MA, Duff A, Weg JG, Fulkerson WJ, Palevsky HI, et al. The clinical course of pulmonary embolism. N Engl J Med. 1992. 326:1240–1245.
4. Nijkeuter M, Hovens MM, Davidson BL, Huisman MV. Resolution of thromboemboli in patients with acute pulmonary embolism: a systematic review. Chest. 2006. 129:192–197.
5. Goldhaber SZ. Bonow RO, Mann DL, Zipes DP, Libby P, Braunwald E, editors. Pulmonary embolism. Braunwald's heart disease: a textbook of cardiovascular medicine. 2012. 9th ed. Philadelphia: Saunders;1679–1695.
6. Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galié N, Pruszczyk P, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008. 29:2276–2315.
7. Yong HS. MDCT application in the Vascular System. J Korean Med Assoc. 2007. 50:25–32.
8. Aujesky D, Obrosky DS, Stone RA, Auble TE, Perrier A, Cornuz J, et al. Derivation and validation of a prognostic model for pulmonary embolism. Am J Respir Crit Care Med. 2005. 172:1041–1046.
9. Choi WH, Kwon SU, Jwa YJ, Kim JA, Choi YH, Chang JH, et al. The pulmonary embolism severity index in predicting the prognosis of patients with pulmonary embolism. Korean J Intern Med. 2009. 24:123–127.
10. Gans H, Rosenberg M, Tan BH, Boulton A. The mechanism of spontaneous resolution of thromboemboli. Surg Gynecol Obstet. 1970. 130:326–332.
11. Wilson JE 3rd, Frenkel EP, Pierce AK, Johnson RL Jr, Winga ER, Curry GC, et al. Spontaneous fibrinolysis in pulmonary embolism. J Clin Invest. 1971. 50:474–480.
12. Walker RH, Goodwin J, Jackson JA. Resolution of pulmonary embolism. Br Med J. 1970. 4:135–139.
13. Geerts WH, Heit JA, Clagett GP, Pineo GF, Colwell CW, Anderson FA Jr, et al. Prevention of venous thromboembolism. Chest. 2001. 119:1 Suppl. 132S–175S.
14. Shinohara Y, Nishimaru K, Sawada T, Terashi A, Handa S, Hirai S, et al. Sarpogrelate-aspirin comparative clinical study for efficacy and safety in secondary prevention of cerebral infarction (S-ACCESS): a randomized, double-blind, aspirin-controlled trial. Stroke. 2008. 39:1827–1833.
 XML Download
XML Download