

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Acute lung injury (ALI) may occur secondary to an extensive number of direct or indirect pulmonary insults and consequently results in hypoxic respiratory failure1. Most cases of clinical ALI will show a specific histological feature, diffuse alveolar damage (DAD). In 2002, Beasley et al.2 reported acute fibrinous and organizing pneumonia (AFOP) as an unusual type of ALI. The histological pattern of AFOP is differentiated from DAD by the absence of hyaline membranes, and from eosinophilic pneumonia (EP) by the lack of eosinophils. They noted several conditions associated with AFOP, including collagen-vascular diseases, malignancies, drugs, and infections. However, few cases of AFOP have been reported until now in Korea. Herein, we report an extraordinary case of AFOP in a healthy patient.
Case Report
Patient: A 49-year-old female.
Chief complaint: Worsening of dyspnea on exertion for one month.
Present illness: A 49-year-old female visited our hospital emergency room (ER) due to worsening of dyspnea. Four weeks ago, she slept under a home ultrasonic humidifier turned on, containing sterilizer for several days. After several days of that event, she developed dry cough and dyspnea on exertion. She visited another hospital and checked the chest radiography. The considerable differential diagnoses were bronchiolitis obliterans with organizing pneumonia (BOOP) or nonspecific interstitial pneumonia (NSIP). She was given oral prednisone (60 mg/day) and empirical antibiotics for about three weeks, but suffered a progressive worsening of dyspnea.
Past medical history: The patient had no specific past medical history.
Social history: The patient had no history of smoking and alcohol consumption.
Physical examination: At ER, the patient was alert with a body temperature of 98.8°F, heart rate of 96 beats/min, respiratory rate of 22/min, blood pressure of 116/74 mm Hg and oxygen saturation at 80.2% on room air. There was no fever or peripheral edema. Cardiac and abdominal examinations were normal. Lung auscultation revealed fine inspiratory crackles in both basal lung fields.
Initial laboratory findings: Complete blood cell count showed a white blood cell count of 15.13×103/µL (normal, 4.0~10.0×103/µL), a hemoglobin concentration of 15.0 g/dL (normal, 14~18 g/dL), and a platelet count 282×103/µL (normal, 130~450×103/µL). The differential count showed neutrophils at 67%, lymphocytes at 21%, and monocytes at 8.3%. The C-reactive protein level was 1.1 mg/dL (normal, ≤0.5 mg/dL). Her serum sodium, potassium, creatinine, magnesium, calcium, and liver function test were all within normal limits. Blood and sputum cultures and gram staining were all negative. Urinary S. pneumoniae Ag was negative.
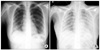
Radiologic findings: The initial chest radiography showed diffuse fine reticular and nodular opacities in both lungs (Figure 1A). The chest radiograph after intubation and application of mechanical ventilation changed the progression of initial findings with diffuse consolidations (Figure 1B). Chest computed tomography scan at ER demonstrated patchy consolidations with fibrosis in the right lower lobe and ill-defined centrilobular ground glass opacity in the both lungs (Figure 2).
Bronchoscopic findings: Bronchoscopy on first day of hospitalization did not reveal any endobronchial lesions or abnormal secretions. Bronchioalveolar lavage (BAL) was done in the right lower lobe postero-basal segment. Microbiologic cultures for common respiratory virus, bacteria and fungus containing Pneumocystis jirovecii were all negative. The BAL fluid consisted of 34% macrophages, 30% neutrophils, and 16% lymphocytes. There was no evidence of malignant cells.
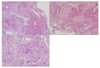
Pathological findings: The pathological finding showed patchy areas of lung parenchymal by fibrin deposits in the alveolar ducts and alveoli. The lung parenchyma shows intra-alveolar spaces containing fibrous plugging with extensive fibrin deposition, a finding consistent with cryptogenic organizing pneumonia with fibrous exudates. Fibrin balls with hemosiderin deposition are noted in the alveolar spaces (Figure 3). The characteristic intra-alveolar fibrin ball and lack of hyaline membrane are the predominant histological features of AFOP.
Hospital course: On first hospital day, the patient developed a respiratory rate of 40 per min after the bronchoscopy and a high fever up to 103.1°F and the demand for oxygen increased. Thus, she was started on broad spectrum antibiotics including 3rd cephalosporin and quinolone. Additionally, she transferred to the medical intensive care unit for close monitoring. She subsequently required intubation and started on mechanical ventilator care.
On second hospital day, the patient underwent wedge biopsies of the right upper lobe and right lower lobe through the video-assisted thoracoscopic surgery (VATS). After establishing the diagnosis of AFOP, the patient was started on intravenous corticosteroid pulse therapy (methylprednisolone, 1 g/day) for three days and continued with maintenance therapy (60 mg/day). However, the PaO2/FiO2 ratio gradually decreased with an increase in ventilator requirements (FiO2 0.95). The arterial blood gas analysis showed permissive hypercapnia (PaO2 75.7, PCO2 51.4, pH 7.252). The patient could not be weaned off the ventilator and chest radiograph was aggravated, and nitric oxide gas was applied after all.
On 4th hospital day, the family of the patient consented to wait for a lung transplantation and an extracorporeal membrane oxygenator (ECMO) was inserted to her due to persistent hypoxemia and hypercapnia under full ventilator settings. However, during the vascular procedure, the patients lost massive amounts of arterial blood and went into hypovolemic shock. The patient was successfully resuscitated from hypovolemic shock. But the patient's hospital course deteriorated rapidly.
On 9th hospital day, the family of the patient refused to wait for a lung transplantation and wanted removal of ECMO. On 13th hospital day, she died due to respiratory failure and multiple organ failure.
Discussion
AFOP was first described by Beasley et al. in 20022. In their paper, tissue histopathology of AFOP revealed intra-alveolar fibrin in the form of fibrin balls and organizing pneumonia with patchy distributions1,2. The differential diagnosis of AFOP is primarily with DAD and EP. The AFOP pattern differs from that of DAD in that the fibrin is organized into balls within the alveolar spaces and classic hyaline membranes are not seen. And the histological pattern of AFOP differs from the pattern of EP by the lack of prominent eosinophils2.
Since it is difficult to diagnose AFOP by small biopsy, a confident diagnosis of AFOP requires surgical lung biopsy 2. In our case, VATS biopsy was done and the pathological findings showed patchy areas of the lung parenchyma by fibrin deposits in the alveolar ducts and alveoli. Fibrin ball is a characteristic finding of AFOP and presented as dense and red coalescent masses on hematoxylin-eosin (H&E) staining. Finally, there was no evidence of hyaline membranes in alveoli in our case, the final pathologic diagnosis was consistent with AFOP.
In previous studies about AFOP, the onset of dyspnea and non-productive cough of less than two months duration were observed. Moreover, the most common radiological findings of AFOP showed bilateral basilar infiltrates2. In this case, the patient had similar symptoms and radiological findings. In addition, AFOP has been associated with infections, connective tissue disorders, occupational hazards, drug exposures, and so on2-5. Recently, additional cases of AFOP have been reported in patients with HIV and Pneumocystis jirovecii pneumonia, hematopoetic stem cell transplantation, and systemic lupus erythematosus6-8.
However, some patients had no identifiable predisposing condition or association with AFOP2. Our patient did not appear to be associated with any known significant exposures or past medical diseases. However, one possibility of exposure was the home ultrasonic humidifier, which contained a sterilizer. For several days, the patient slept with the humidifier turned on, and the symptoms of dyspnea on exertion and cough appeared a few days later. In some previous studies, humidifiers have been associated with inhalation lung injury, for example, hypersensitivity pneumonitis9,10. And some cases were reported about humidifier-associated diseases like extrinsic allergic alveolitis and toxic aveolitis11,12. However, it is not clear that humidifier have been associated with AFOP in this case.
The prognosis of AFOP appears to have two distinct patterns of disease progression: one is a fulminant illness with rapid progression to death and the other is a subacute and, less fulminate course from which the patient recovers eventually2. Approximately, 30% of patients with AFOP require mechanical ventilation and all patients who needed mechanical ventilation died. Overall, AFOP showed poor prognosis with up to 50% mortality2.
Some previous case reports showed the successful treatment of AFOP with corticosteroid and immunosuppressant agents13-15, such as the combination of cyclophosphamide and prednisone13 or mycophenolate and methylprednisolone14. In our case, the patient was treated with intravenous corticosteroid pulse therapy (methylprednisolone, 1 g/day) for three days. However, the clinical course was aggravated and lung transplantation was planed. Despite the proper treatment for AFOP, the patient had a poor response and outcome to steroid therapy.

 XML Download
XML Download