

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Streptococcus parasanguinis is a Viridans group bacteria that is most often discovered in the oral cavity and causes dental plaque and endocarditis in a rat model. It has low virulence but an unknown relationship to human respiratory infections. We report on a 61-year-old woman who developed hemoptysis followed by pleuritic chest pain after conscious sedation during a gastroscopic polypectomy and was diagnosed with pneumonia and parapneumonic effusion from Streptococcus parasanguinis isolated in pleural fluid. Microaspiration during the procedure was presumed to play a role in the pathogenesis.
Figures and Tables
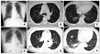 | Figure 1Chest PA view and chest CT. (A) Chest PA at a local clinic shows no active lung lesion. (B, C) Chest CT at a local clinic shows ill defined nodules in the posterior segment of the right upper lobe with patchy ground glass opacity in the posterobasal segment of the right lower lobe. (D) Chest PA on admission. Focal consolidation is seen in the right lower lung field. (E, F) Chest CT on admission shows increased extent of consolidation with ground glass opacity in the right lower lobe and a small volume of pleural effusion in a right-sided hemithorax. PA: posterior anterior; CT: computed tomography.
|
 | Figure 2Chest PA view and chest CT. (A) Chest PA on day 9 of admission. Improved consolidation and an increased volume of pleural effusion is shown in the right lung. (B~D) Chest CT on day 9 of admission. Near complete clearing of the previous consolidation in the posterobasal segment of the right lower lung and increased volume of pleural effusion, which was considered a hemothorax, is shown. (E) Chest PA about 3 months after discharge. Decreased volume of pleural effusion is shown compared with that of day 9 from admission. (F~H) Chest CT about 3 months after discharge shows neither pleural effusion nor consolidation. PA: posterior anterior; CT: computed tomography.
|
References
1. Facklam R. What happened to the streptococci: overview of taxonomic and nomenclature changes. Clin Microbiol Rev. 2002. 15:613–630.
2. Wilson WR, Karchmer AW, Dajani AS, Taubert KA, Bayer A, Kaye D, et al. Antibiotic treatment of adults with infective endocarditis due to streptococci, enterococci, staphylococci, and HACEK microorganisms. American Heart Association. JAMA. 1995. 274:1706–1713.
3. Bochud PY, Calandra T, Francioli P. Bacteremia due to viridans streptococci in neutropenic patients: a review. Am J Med. 1994. 97:256–264.
4. Han XY, Kamana M, Rolston KV. Viridans streptococci isolated by culture from blood of cancer patients: clinical and microbiologic analysis of 50 cases. J Clin Microbiol. 2006. 44:160–165.
5. Jenkinson HF, Lamont RJ. Streptococcal adhesion and colonization. Crit Rev Oral Biol Med. 1997. 8:175–200.
6. Burnette-Curley D, Wells V, Viscount H, Munro CL, Fenno JC, Fives-Taylor P, et al. FimA, a major virulence factor associated with Streptococcus parasanguis endocarditis. Infect Immun. 1995. 63:4669–4674.
7. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007. 44:Suppl 2. S27–S72.
8. File TM. Community-acquired pneumonia. Lancet. 2003. 362:1991–2001.
9. Davies CW, Kearney SE, Gleeson FV, Davies RJ. Predictors of outcome and long-term survival in patients with pleural infection. Am J Respir Crit Care Med. 1999. 160:1682–1687.
10. Tsang KY, Leung WS, Chan VL, Lin AW, Chu CM. Complicated parapneumonic effusion and empyema thoracis: microbiology and predictors of adverse outcomes. Hong Kong Med J. 2007. 13:178–186.
11. Paik S, Senty L, Das S, Noe JC, Munro CL, Kitten T. Identification of virulence determinants for endocarditis in Streptococcus sanguinis by signature-tagged mutagenesis. Infect Immun. 2005. 73:6064–6074.
12. Komatsu K, Kanda T. Atypical lung abscess occurring in an elderly female suffering from diabetes mellitus--a case report. Kansenshogaku Zasshi. 1997. 71:260–263.
13. Fernández-Garayzábal JF, Fernández E, Las Heras A, Pascual C, Collins MD, Domínguez L. Streptococcus parasanguinis: new pathogen associated with asymptomatic mastitis in sheep. Emerg Infect Dis. 1998. 4:645–647.
14. Reisz G, Stevens D, Boutwell C, Nair V. The causes of hemoptysis revisited. A review of the etiologies of hemoptysis between 1986 and 1995. Mo Med. 1997. 94:633–635.
15. El-Solh AA, Pietrantoni C, Bhat A, Aquilina AT, Okada M, Grover V, et al. Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med. 2003. 167:1650–1654.
 XML Download
XML Download