

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
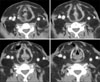
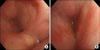
Multiple symmetrical lipomatosis (MSL), also called Madelung's disease, is a rare disorder of unknown etiology and characterized by abnormal accumulation of large subcutaneous fatty masses in neck, shoulder, and upper trunk. MSL has known to predominantly affect middle-aged men with a history of alcoholism. Although the clinical course of MSL is considered to be slowly progressive, in advanced stage, fatty masses in the neck may compress the upper aerodigestive tract, resulting in dyspnea and dysphagia. The treatment of MSL is surgical resection, but radical excision is very difficult and recurrence after surgery is frequent. We report the case of 55-year-old man with long lasting MSL, which caused severe airway obstruction. This patient was admitted with progressive dyspnea and massive accumulation of fat around the vocal cord that was detected on a neck CT scan. This abnormal fatty infiltration in supraglottic region caused upper airway obstruction.
Figures and Tables
Figure 1
Anterior (A) and lateral (B) view of the patient show multiple, symmetric subcutaneous fatty masses in neck, shoulder and upper trunk.

Figure 2
(A) Chest AP shows widening of superior mediastinum. (B) Chest CT shows compression and displacement of the trachea by surrounding fat infiltration in mediastinum and bilateral pleural effusions.

References
1. Meningaud JP, Pitak-Arnnop P, Bertrand JC. Multiple symmetric lipomatosis: case report and review of the literature. J Oral Maxillofac Surg. 2007. 65:1365–1369.
2. Enzi G. Multiple symmetric lipomatosis: an updated clinical report. Medicine (Baltimore). 1984. 63:56–64.
3. Enzi G, Busetto L, Ceschin E, Coin A, Digito M, Pigozzo S. Multiple symmetric lipomatosis: clinical aspects and outcome in a long-term longitudinal study. Int J Obes Relat Metab Disord. 2002. 26:253–261.
4. Hirose A, Okada Y, Morita E, Tanaka Y. Benign symmetric lipomatosis associated with alcoholism. Intern Med. 2006. 45:1001–1005.
5. Lee HW, Kim TH, Cho JW, Ryu BY, Kim HK, Choi CS. Multiple symmetric lipomatosis: Korean experience. Dermatol Surg. 2003. 29:235–240.
6. Yoon SM, Kim YS, Kim JH, Lee DS, Choi JW, Yang SC, et al. A case of multiple symmetric lipomatosis. Tuberc Respir Dis. 1999. 47:97–102.
7. Ko MJ, Chiu HC. Madelung's disease and alcoholic liver disorder. Hepatology. 2010. 51:1466–1467.
8. Milisavljevic D, Zivic M, Radovanović Z, Stankovic P. Severe dyspnea as atypical presenting symptom of Madelung's disease. Hippokratia. 2010. 14:133–135.
9. Kwon SH, Kim SC, Seo HS, Choi HS. Surgical treatment of two cases of benign symmetrical lipomatosis causing dyspnea. Korean J Otolaryngol-Head Neck Surg. 2006. 49:758–762.
10. González-García R, Rodréguez-Campo FJ, Sastre-Pérez J, Muñoz-Guerra MF. Benign symmetric lipomatosis (Madelung's disease): case reports and current management. Aesthetic Plast Surg. 2004. 28:108–112.
11. Morinaka S, Sato T, Miyoshi H, Iwashita K. A case of multiple symmetrical lipomatosis (Madelung's disease). Auris Nasus Larynx. 1999. 26:349–353.
12. Gámez J, Playán A, Andreu AL, Bruno C, Navarro C, Cervera C, et al. Familial multiple symmetric lip omatosis associated with the A8344G mutation of mitochondrial DNA. Neurology. 1998. 51:258–260.
13. Faga A, Valdatta LA, Thione A, Buoro M. Ultrasound assisted liposuction for the palliative treatment of Madelung's disease: a case report. Aesthetic Plast Surg. 2001. 25:181–183.
14. Uglesić V, Knezević P, Milić M, Jokić D, Kosutić D. Madelung syndrome (benign lipomatosis): clinical course and treatment. Scand J Plast Reconstr Surg Hand Surg. 2004. 38:240–243.
 XML Download
XML Download