

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Open lung biopsy is used for diagnosis of diffuse infiltrative lung diseases (DILD), but it is invasive and relatively expensive procedure. Fluoroscopy-guided cutting needle lung biopsy (FCNLB) has merits of avoidance of admission and rapid diagnosis. But diagnostic accuracy and safety were not well known in the diagnosis of DILD.
Methods
We included 52 patients (37 men, 15 women) having DILD on HRCT with dyspnea, except the patients who could be confidently diagnosed with clinical and HRCT findings. FCNLB was performed using 16G Ace cut needle (length 1.5 cm, diameter 2 mm) at the area of most active lesion on HRCT. Final diagnoses were made by the consensus.
Results
The mean interval between the HRCT and FCNLB was 4.5 days. Most cases were performed one biopsy during 5~10 minutes. Specific diagnosis was obtained in 43 of 52 biopsies (83%). The most common diagnosis was nonspecific interstitial pneumonia (11 cases) and followed by cryptogenic organizing pneumonia (7 cases), diffuse alveolar hemorrhage and usual interstitial pneumonia (5 cases in each), hypersensitivity pneumonitis (3 cases), tuberculosis and drug induced interstitial pneumonitis (2 cases in each), the others are in one respectively. Mild complication was developed in 9 patients (8 pneumothorax, 1 hemoptysis). Most of complications were regressed without treatment except one case with chest tube insertion for pneumothorax.
Figures and Tables
Figure 1
HRCT axial image & CT scanogram. The most adequate biopsy site was decided on axial scan (short bar), and matched with CT scanogram (black line). This biopsy site was been marking on patient chest wall under the fluoroscopy (arrow).
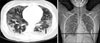

Figure 3
Thirty eight year old female patient complaining with coughing, mild fever and dyspnea for one month. (A) HRCT shows bilateral diffuse subpleural consolidation and ground glass opacity in entire lung. Cutting needle biopsy site was decided at the subpleural lesion of LLL posterobasal segment (short bar). (B) Pathologic finding of 16 G cutting needle lung biopsy specimen demonstrated diffuse even infiltration of chronic inflammatory cells in interstitium indicative of cellular nonspecific interstitial pneumonia (H&E stain, ×400).

Figure 4
Sixty four year old woman complaining slowly progressing dyspnea for 4 years. (A) HRCT shows bilateral diffuse peribronchial and subpleural ground glass opacities and some consolidation with variable sized air-containing cysts. Biopsy site was decided at the subpleural lesion of RUL anterior segment (short bar). (B) Pathologic specimen demonstrated dense lymphoplasma cell infiltration in interstitium of the lung, compatible with lymphocytic interstitial pneumonia (H&E stain, ×400).

Figure 5
Thirty two year old woman with mild fever and dyspnea during 3 days. (A) HRCT shows bilateral lobar or segmental consolidation and surrounding ground glass opacities. We suggested pneumonia and antibiotic therapy was started but without response. Fluoroscopy-guided cutting needle biopsy site was RLL posterobasal segment (short bar). (B) Cutting needle lung biopsy specimen demonstrated prominent eosinophil infiltration in interstitium and intraalveolar space, indicative of eosinophilic pneumonia (H&E stain, ×400). Churg-Strauss syndrome was diagnosed considering clinical finding with bronchial asthma and peripheral eosinophilia.
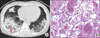
Figure 6
(A) HRCT demonstrated bilateral diffuse multiple small round nodules especially peripheral lung zone, suggesting lung metastasis. But primary malignancy was not found and cutting needle biopsy was decided (short bar). (B) Cutting needle biopsy specimen demonstrated multiple intra-alveolar fibroblast plug (arrow), diagnosed with cryptogenic organizing pneumonia (H&E stain, ×100).


References
1. Ferguson MK. Thoracoscopy for diagnosis of diffuse lung disease. Ann Thorac Surg. 1993. 56:694–696.
2. McElvein RB. The surgical approach to interstitial lung disease. Clin Chest Med. 1982. 3:485–490.
3. Arora VK, Gupta R, Johri A. Open lung biopsy in diffuse infiltrative lung disease with progressive dyspnoea: is it useful? Indian J Chest Dis Allied Sci. 2002. 44:203–206.
4. Meyer KC. The role of bronchoalveolar lavage in interstitial lung disease. Clin Chest Med. 2004. 25:637–649.
5. Herf SM, Suratt PM, Arora NS. Deaths and complications associated with transbronchial lung biopsy. Am Rev Respir Dis. 1977. 115:708–711.
6. Wall CP, Gaensler EA, Carrington CB, Hayes JA. Comparison of transbronchial and open biopsies in chronic infiltrative lung diseases. Am Rev Respir Dis. 1981. 123:280–285.
7. Lee JH, Lee JC, Kwon JT. Surgical lung biopsy for diffuse infiltrative lung disease. Korean J Thorac Cardiovasc Surg. 2006. 39:844–849.
8. Niden AH, Salem F. A safe high-yield technique for cutting needle biopsy of the lung in patients with diffuse lung disease. Chest. 1997. 111:1615–1621.
9. Jang I, Kim SW, Yahang JH, Kim JW, Choi JY, Rhie S. Thoracic surgeon's role in differential diagnosis of the interstitial lung disease. Korean J Thorac Cardiovasc Surg. 2006. 39:382–386.
10. Klassen KP, Andrews NC. Biopsy of diffuse pulmonary lesions. A seventeen-year experience. Ann Thorac Surg. 1967. 4:117–124.
11. Flint A, Martinez FJ, Young ML, Whyte RI, Toews GB, Lynch JP 3rd. Influence of sample number and biopsy site on the histologic diagnosis of diffuse lung disease. Ann Thorac Surg. 1995. 60:1605–1607.
12. Manhire A, Charig M, Clelland C, Gleeson F, Miller R, Moss H, et al. Guidelines for radiologically guided lung biopsy. Thorax. 2003. 58:920–936.
13. Yankelevitz DF, Vazquez M, Henschke CI. Special techniques in transthoracic needle biopsy of pulmonary nodules. Radiol Clin North Am. 2000. 38:267–279.
14. Murphy JM, Gleeson FV, Flower CD. Percutaneous needle biopsy of the lung and its impact on patient management. World J Surg. 2001. 25:373–379.
15. Richardson CM, Pointon KS, Manhire AR, Macfarlane JT. Percutaneous lung biopsies: a survey of UK practice based on 5444 biopsies. Br J Radiol. 2002. 75:731–735.
16. Glassberg RM, Sussman SK. Life-threatening hemorrhage due to percutaneous transthoracic intervention: importance of the internal mammary artery. AJR Am J Roentgenol. 1990. 154:47–49.
 XML Download
XML Download