

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Epithelioid sarcomas are very rare soft tissue sarcoma that comprises less than 1% of all soft tissue sarcomas1. In 1970, Enzinger gave the name epithelioid sarcoma to a group of soft-tissue sarcomas that were often confused with a chronic inflammatory process, a necrotizing granuloma, or a squamous-cell carcinoma2. Long term studies showed that 40~57% of patients with epithelioid sarcoma developed metastasis3-5. The lung is the most common site for dissemination5. Other frequent sites include lymph node and scalp3,5,6. The trunk, perineum, spine, penis, and vulva also have been occasionally reported as other sites of metastasis6.
Although the frequency of endobronchial metastasis varies according to definition (from 2% to 28%)7,8, the incidence of clinically significant metastasis of major bronchus from extrathoracic tumors occurs in 2% to 5% of all cases7. The common extrathoracic malignancies include breast, colorectal, and renal carcinoma7. There have been only a few reports on endobronchial metastasis from soft tissue sarcoma9,10. Especially, there has been no report on endobronchial metastasis from epithelioid sarcoma to our knowledge. This is the first report on epithelioid sarcoma with endobronchial metastasis diagnosed by bronchoscopic and muscle biopsy.
Case Report
A 28-year-old man presented with chest pain and dyspnea in June 2008. Simple chest radiography and chest computed tomography (CT) revealed bilateral pneumothorax. He underwent bilateral wedge resection by Video-Assisted Thoracoscopic Surgery (VATS) and the histologic diagnosis was 'ruptured alveolar septa with granulomatous inflammation'. He underwent right thoracotomy in May 2009 due to recurred pneumothorax. Histologic examination of the lung, pleura and multiple lymph nodes showed only chronic inflammation with granuloma. His physician couldn't identify the cause for recurrent pneumothorax.
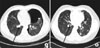
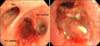
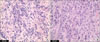
In July 2009, he presented with chest pain and dyspnea to Seoul National University Hospital. He complained of hemoptysis, 3 month history of chronic cough, and 2 week history of swelling of left thigh. On physical examination, breath sound was decreased over left lung field and several small, hard, painless nodules in the left thigh were noticed. Routine laboratory test was unremarkable. Chest CT on admission showed left pneumothorax, multiple air cysts and nodules in both lungs and endobronchial lesion in right lower basal lobe (Figure 1A). Serial outside CT images revealed that the endobronchial lesion developed newly in March 2009 and has progressed. The multiple lung nodules have aggravated since 2008. Bronchoscopy showed hemorrhagic mass that obstructed the bronchus of right lower basal lobe (Figure 2). Magnetic resonance imaging revealed multiple nodular lesions of variable size in the left thigh muscles. The specimen of bronchoscopic biopsy and left thigh muscle biopsy were composed of relatively uniform, polygonal or epithelioid cells with abundant, deeply eosinophilic cytoplasm, suggesting epithelioid sarcoma (Figure 3).
Immunohistochemical staining for cytokeratin, epithelial membrane antigen, vimentin, and CD34 were all positive (Figure 4), however, S-100, and CD68 were negative. Finally, he was diagnosed with epithelioid sarcoma.
The patient underwent six cycles of combination chemotherapy with ifosfamide, cisplatin and etoposide from August 2009 to December 2009. While the endobronchial lesion disappeared in chest CT (Figure 1B), the MRI of lower extremity showed progression of the multiple nodules in the left thigh in January 2010. In the left occipital area there was a growing ulcerative lesion, which turned out to be epithelioid sarcoma. Consequently, a progressive disease was diagnosed and the chemotherapy regimen was switched to combination chemotherapy consisting of ifosfamide and adriamycin. He has received additional 4 cycles of chemotherapy so far.
Discussion
Epithelioid sarcomas are rare subtype of soft tissue sarcoma and have unclear histogenesis. The incidence of epitheloid carcoma is increasing, with a annual percentage change of 5.2% since 1973. In 2005, the incidence is estimated 0.4 case per million11. Epithelioid sarcoma affects mainly the subcutaneous tissues, fascia, or tendon sheaths of the extremities. There is a preponderance of upper than the lower extremities. Clinically, the tumor usually starts as a painless, slowly growing mass, but not uncommonly presents as a multifocal lesion. The superficial lesions are often ulcerated. Young adults aged between 20 and 40 years old are mostly affected. There is a preponderance for male gender (2:1)2,12.
It is often difficult to diagnose the epithelioid sarcoma. Histologically the sarcoma can be confused with a variety of benign and malignant conditions, including chronic inflammatory processes, granuloma, synovial sarcoma, and ulcerating squamous cell carcinoma2. Since the diagnosis is difficult, a definitive diagnosis is often delayed. Ross et al reported that the mean interval between the onset of symptoms and definitive diagnosis was 18 months6 and other study showed that the median interval between observing the initial symptoms, making a diagnosis, and starting treatment was 3.5 months, ranging between 1 month and 36 months5. In the present case, we needed 13 months from onset of symptom to histological diagnosis of epithelioid sarcoma.
Epitheloid sarcoma is a high grade tumor with a high local recurrence and metastasis rate. The local recurrence rate ranges between 50~70%5,6, and the metastasis rate between 40~57%3-5. Unlike other soft tissue sarcomas (2.6%), the rate of lymph node involvement is remarkably high. The common metastasis sites include the lung (51%) regional lymph nodes (34%), scalp (22%), and bone (13%).
There have been only a few reports on endobronchial metastasis from soft tissue sarcoma including angiosarcomna and leiomyosarcoma9,10. Although the lung is the most common site of metastasis, only lung parenchyma is typically involved. An endobronchial metastasis of epithelioid sarcoma has not been reported yet.
Wide surgical resection is recommended as treatment of choice5 due to the high local recurrence and metastasis rate of epithelioid sarcoma. High-dose chemoradiotherapy can also achieve low local recurrence rates6,13,14. In general, the treatment of endobronhial metastasis is determined by the histology and location of the primary tumor and other metastasis sites, as well as the patients' performance status15. The majority of patients with endobronchial metastasis have metastasis to other sites other than endobronchial tree. Therefore most patients are treated with systemic chemotherapy. But in patients with localized disease, surgical resection can be considered15.
Our patient has been treated with systemic chemotherapy since he had multiple nodules in the thigh with multiple lung metastasis at the time of diagnosis. Although endobronchial lesion disappeared after six cycles of chemotherapy, lung metastasis increased so that his overall disease status was "progressive disease."
In epithelioid sarcoma, advanced age, male gender, proximal or axial location, depth, tumor size, mitotic figures, necrosis, vascular invasion, and tumor hemorrhage have been identified as adverse prognostic factors11. In addition, local recurrence, lymph node metastasis, and the extent of surgery were also associated with survival in some studies6,11,12. The 5-year overall survival ranges between 60% and 75%3,6,11. In summary, we report the first case of epithelioid sarcoma with endobronchial metastasis, confirmed by bronchoscopic biopsy. Although our patient underwent wedge resection of the lung three times, we could not timely diagnose the epitheolid sarcoma with endobronchial metastasis. Because epitheloid sarcoma can be easily confused with chronic inflammatory processes and granuloma, a correct pathologic diagnosis by an experienced pathologist is essential.

 XML Download
XML Download