

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Social welfare services for respiratory-disabled persons in Korea are offered based on the respiratory impairment grade, which is determined by 3 clinical parameters; dyspnea, forced expiratory volume in 1 second (FEV1), and arterial oxygen tension. This grading system has several limitations in the objective assessment of respiratory impairment. We reviewed several guidelines for the evaluation of respiratory impairment and relevant articles. Then, we discussed a new grading system with respiratory physicians. Both researchers and respiratory physicians agreed that pulmonary function tests are essential in assessing the severity of respiratory impairment, forced vital capacity (FVC), FEV1 and single breath diffusing capacity (DLco) are the primarily recommended tests. In addition, we agreed that arterial blood gas analysis should be reserved for selected patients. In conclusion, we propose a new respiratory impairment grading system utilizing a combination FVC, FEV1 and DLco scores, with more social discussion included.
Figures and Tables

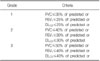
Table 2
Respiratory impairment grading according to guidelines of the Korean Academy of Medical Science6

Table 3
American Thoracic Society impairment categories, with corresponding description of ability to perform job demands8


References
1. Choi MY. Health and medical care for people with disability. Health Welf Policy Forum. 2009. 153:46–63.
2. World Health Organization. International classification of impairment, activity and participation (ICIDH-2). 1980. Geneva, Switzerland: World Health Organization.
3. Welfare of Disabled Persons Act. Korea Ministry of Government Legislation. c1997-2011. cited 2011 Mar 10. Available from: http://www.law.go.kr/main.html.
4. Ministry of Health and Welfare (Korea). Bulletin 2000-37. 2003. Seoul: Ministry of Health and Welfare.
5. Kyung SY, Kim YJ, An CH, Lee SP, Park JW, Jeong SH. Clinical findings of the patients with legal pulmonary disability: short-term follow-up at a tertiary university hospital in Korea. Korean J Intern Med. 2008. 23:72–77.
6. Kim H, Lee KY, Kim JT, Uh ST. Committee on Respiratory Impairment. Korean Academy of Medical Sciences. Guideline of the Korean Academy of Medical Sciences for assessing respiratory impairment. J Korean Med Sci. 2009. 24:Suppl 2. S267–S270.
7. American Thoracic Society, medical section of the American Lung Association. Evaluation of impairment/disability secondary to respiratory disease. Am Rev Respir Dis. 1982. 126:945–951.
8. Evaluation of impairment/disability secondary to respiratory disorders. disability secondary to respiratory disorders. American Thoracic Society. Am Rev Respir Dis. 1986. 133:1205–1209.
9. Cocchiarella L, Andersson GBJ. Guides to the evaluation of permanent impairment. 2001. 5th ed. Chicago: American Medical Association.
10. Becklake MR, Rodarte JR, Kalica AR. NHLBI workshop summary. Scientific issues in the assessment of respiratory impairment. Am Rev Respir Dis. 1988. 137:1505–1510.
11. Epstein P. Fishman AP, Elias JA, Senior RM, Fishman JA, Pack AI, Grippi MA, editors. Evaluation of impairment and disability due to lung disease. Pulmonary diseases and disorders. 2008. 4th ed. New York, NY: McGraw-Hill;677–690.
12. Mayer AS, Maier L. Adams L, Ayas N, Alberg A, Blkissoon RC, Albert R, Albertine KH, editors. Evaluation of respiratory impairment and disability. Murray and Nadels Textbook of Respiratory Medicine 1. 2010. 5th ed. Philadelphia, PA: Saunders;591–610.
13. Malley WJ. Clinical blood gases: assessment and intervention. 2005. 2nd ed. St. Louis, Mo: Elsevier Saunders.
14. Cerveri I, Zoia MC, Fanfulla F, Spagnolatti L, Berrayah L, Grassi M, et al. Reference values of arterial oxygen tension in the middle-aged and elderly. Am J Respir Crit Care Med. 1995. 152:934–941.
15. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005. 26:319–338.
16. Macintyre N, Crapo RO, Viegi G, Johnson DC, van der Grinten CP, Brusasco V, et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur Respir J. 2005. 26:720–735.
17. Kanner RE, Renzetti AD Jr, Stanish WM, Barkman HW Jr, Klauber MR. Predictors of survival in subjects with chronic airflow limitation. Am J Med. 1983. 74:249–255.
18. Traver GA, Cline MG, Burrows B. Predictors of mortality in chronic obstructive pulmonary disease. A 15-year follow-up study. Am Rev Respir Dis. 1979. 119:895–902.
19. Anthonisen NR, Wright EC, Hodgkin JE. Prognosis in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1986. 133:14–20.
20. Tockman MS, Comstock GW. Respiratory risk factors and mortality: longitudinal studies in Washington County, Maryland. Am Rev Respir Dis. 1989. 140:S56–S63.
21. Foxman B, Higgins IT, Oh MS. The effects of occupation and smoking on respiratory disease mortality. Am Rev Respir Dis. 1986. 134:649–652.
22. Ortmeyer CE, Costello J, Morgan WK, Swecker S, Peterson M. The mortality of Appalachian coal miners, 1963 to 1971. Arch Environ Health. 1974. 29:67–72.
23. Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007. 176:532–555.
24. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005. 26:948–968.
25. Kannel WB, Hubert H, Lew EA. Vital capacity as a predictor of cardiovascular disease: the Framingham study. Am Heart J. 1983. 105:311–315.
26. Kannel WB, Lew EA, Hubert HB, Castelli WP. The value of measuring vital capacity for prognostic purposes. Trans Assoc Life Insur Med Dir Am. 1980. 64:66–83.
27. Epler GR, Saber FA, Gaensler EA. Determination of severe impairment (disability) in interstitial lung disease. Am Rev Respir Dis. 1980. 121:647–659.
28. Neas LM, Schwartz J. Pulmonary function levels as predictors of mortality in a national sample of US adults. Am J Epidemiol. 1998. 147:1011–1018.
29. Ferguson MK, Little L, Rizzo L, Popovich KJ, Glonek GF, Leff A, et al. Diffusing capacity predicts morbidity and mortality after pulmonary resection. J Thorac Cardiovasc Surg. 1988. 96:894–900.
30. Ferguson MK, Vigneswaran WT. Diffusing capacity predicts morbidity after lung resection in patients without obstructive lung disease. Ann Thorac Surg. 2008. 85:1158–1164.
31. Choi JK, Paek D, Lee JO. Normal predictive values of spirometry in Korean population. Tuberc Respir Dis. 2005. 58:230–242.
32. Park JO, Choi IS, Park KO. Normal predicted standards of single breath carbon monoxide diffusing capacity of lung in healthy nonsmoking adults. Korean J Intern Med. 1985. 28:176–183.
33. Armstrong BW, Workman JN, Hurt HH Jr, Roemich WR. Clinico-physiologic evaluation of physical working capacity in persons with pulmonary disease. Rationale and application of a method based on estimating maximal oxygen-consuming capacity from MBC and O-2ve. I. Am Rev Respir Dis. 1966. 93:90–99.
34. Roemmich W, Blumenfeld HL, Moritz H. Evaluating remaining capacity to work in miner applicants with simple pneumoconiosis under 65 years of age under Title IV of Public Law 91-173. Ann N Y Acad Sci. 1972. 200:608–616.
35. Wehr KL, Johnson RL Jr. Maximal oxygen consumption in patients with lung disease. J Clin Invest. 1976. 58:880–890.
36. Cotes JE, Posner V, Reed JW. Estimation of maximal exercise ventilation and oxygen uptake in patients with chronic lung disease. Bull Eur Physiopathol Respir. 1982. 18:221–228.
37. Kass I, Dyksterhuis JE, Rubin H, Patil KD. Correlation of psychophysiologic variables with vocational rehabilitation outcome in patients with chronic obstructive pulmonary disease. Chest. 1975. 67:433–440.
 XML Download
XML Download