

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
We report a case of Caplan's Syndrome, which presented as multiple pulmonary nodules. A 58-year-old male was admitted to hospital due to multiple pulmonary nodules. In addition, the patient presented with multiple arthritis, and dyspnea on exertion. Rheumatoid arthritis had been diagnosed 35 years ago. The patient had worked as a stonemason for 20 years. Computed Tomography (CT) revealed numerous well-defined tiny nodules scattered in both lungs, which was suspicious of miliary tuberculosis or malignancy. The patient was started on antituberculous medications and referred to our hospital. First, a transbronchial lung biopsy was performed, which showed no evidence of granuloma. It was our opinion that the biopsy was insufficient, and a follow-up video-associated thoracoscopy was performed. The pathological report determined necrotizing granulomatous inflammation and silicosis on background. According to imaging studies, pathologic reports, and clinical symptoms, we concluded that the patient had Caplan's syndrome. We controlled his rheumatic medications, and instructed him to avoid exposure to hazardous dust.
Figures and Tables

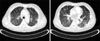
Figure 2
The chest computer tomography (CT) revealed numerous well-defined tiny nodules scattered in both lungs with perilymphatic distribution.


References
1. Caplan A. Certain unusual radiological appearances in the chest of coal-miners suffering from rheumatoid arthritis. Thorax. 1953. 8:29–37.
2. Caplan A. Rheumatoid disease and pneumoconiosis (Caplan's syndrome). Proc R Soc Med. 1959. 52:1111–1113.
3. Verhaeghe A, Voisin C, Grailles M, Delcambre B, Bouscatie F. Developmental aspects of Caplan's syndrome. Rev Rhum Mal Osteoartic. 1969. 36:109–123.
4. Caplan A. Rheumatoid pneumoconiosis syndrome. Med Lav. 1965. 56:494–499.
5. Gough J, Rivers D, Seal RM. Pathological studies of modified pneumoconiosis in coal-miners with rheumatoid arthritis; Caplan's syndrome. Thorax. 1955. 10:9–18.
6. Zielonka TM, Bareła D, Zukowska M, Langfort R, Rudziński P, Chazan R. Caplan's syndrome: case report. Pol Arch Med Wewn. 2005. 114:779–784.
7. Benedek TG. Rheumatoid pneumoconiosis. Documentation of onset and pathogenic considerations. Am J Med. 1973. 55:515–524.
8. Darke C, Wagner MM, Nuki G, Dyer PA. HLA-A, B and DR antigens and properdin factor B allotypes in Caplan's syndrome. Br J Dis Chest. 1983. 77:235–242.
9. Hahon N, Morgan WK, Petersen M. Serum immunoglobulin levels in coal workers' pneumoconiosis. Ann Occup Hyg. 1980. 23:165–174.
10. Payne RB. Serum protein fractions in rheumatoid pneumoconiosis without arthritis. J Clin Pathol. 1962. 15:475–477.
11. Ondrasík M. Caplan's syndrome. Baillieres Clin Rheumatol. 1989. 3:205–210.
12. Allison AC, Harington JS, Birbeck M. An examination of the cytotoxic effects of silica on macrophages. J Exp Med. 1966. 124:141–154.
13. Pernis B. Silica and the immune system. Acta Biomed. 2005. 76:Suppl 2. 38–44.
14. Schreiber J, Koschel D, Kekow J, Waldburg N, Goette A, Merget R. Rheumatoid pneumoconiosis (Caplan's syndrome). Eur J Intern Med. 2010. 21:168–172.
15. Honma K, Vallyathan V. Rheumatoid pneumoconiosis: a comparative study of autopsy cases between Japan and North America. Ann Occup Hyg. 2002. 46:Suppl 1. 265–267.
 XML Download
XML Download