

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Diffuse central airway abnormalities are frequently not apparent or are overlooked on chest radiograph. Recent development of spiral CT techniques with multi-planar reconstructions allows excellent display of central airway anatomy and various abnormalities.
CT relies on the same physical principles as conventional radiography, but CT scan is produced with multiple projections and computed calculations of radiographic density, difference in X-ray absorption so can be displayed in a cross-sectional format. CT scan is the choice of imaging modality for diagnosis of the central airway abnormality and helical CT is preferred because of elimination of slice misregistration and respiratory motion artifacts. With recent development of CT technique, non-axial two-dimensional and three-dimensional reconstructions can be produced with continuous volumetric data set during a single breath-hold. The diagnostic value of reconstruction techniques including multi-planar reconstruction (MPR) or maximum intensity projection (MIP), volume rendering (VR) is most helpful in improving diagnostic confidence and accuracy, particularly for evaluation of obliquely oriented bronchi. Moreover, these reconstruction techniques present anatomic information in an orientation which is more familiar to referring clinicians.
We reviewed various spectrums of diffuse or multicentric airway diseases and arbitrarily classified central airway diseases which are divided into diseases with increased airway luminal diameter and those with decreased diameter (Table 1). We will describe and illustrate various radiographic features of the diffuse abnormalities involving central airways including trachea, main stem bronchi and segmental bronchi focused on spiral CT images with various multi-planar reconstructions.
Diffuse/Multicentric Tracheobronchial Widening
1. Tracheobronchomegaly (Mounier-Kuhn syndrome)
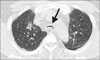
Tracheobronchomegaly shows distinguishable marked dilatation of the trachea and central bronchi and which commonly presents in 4th or 5th decades of men1. The cause of disease is unknown or is thought to result from a congenital deficiency in the internal elastic membrane of the trachea and central bronchi1. An association with Ehlers-Danlos syndrome, Marfan syndrome, and cutis laxa has been described2. The patient presents with repeated respiratory tract infections and associated bronchiectasis.
The diagnosis can be made by measuring the coronal and sagittal diameters of the trachea and bronchi2. Tracheomegaly is defined in women as tracheal diameter greater than 21 mm (coronal) and 23 mm (sagittal) and in men as tracheal diameter greater than 25 mm (coronal) and 27 mm (sagittal). Bronchomegaly is defined in women by diameters of right and left bronchi greater than 20 and 17 mm and in men by diameters greater than 21 and 18 mm, respectively2. There is prolapsed superfluous mucosa through tracheal rings that makes irregular air column ("corrugation") of trachea. The disease is also accompanied by tracheobronchial wall thinning, diverticula and central bronchiectasis on CT scans. Expiratory studies may display collapse of the major airways (Figure 1)1,2.
2. Kartagener syndrome
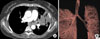
Kartagener syndrome is a subset of primary ciliary dyskinesia syndrome. It has characteristic clinical triad of situs inversus, paranasal sinusitis, bronchiectasis (Figure 2A, B)3,4.
3. Allergic bronchopulmonary aspergillosis (ABPA)
ABPA is a hypersensitivity reaction to antigen of asperogillus fumigatus and related species. Most patients with ABPA have history of asthma or cystic fibrosis and may have associated chronic eosinophilic pneumonia or cryptogenic organizing pneumonia (COP)3. Diagnostic criteria include asthma, peripheral blood eosinophilia, an immediate positive skin test for aspergillus antigens, elevated total serum IgE levels, and increased opacity on chest radiographs3. Acute clinical symptoms present cough, wheezing, low grade fever with malaise, sputum production, and chest pain3.
Characteristic chest radiographic manifestation demonstrate tubular, finger-in-glove increased opacity in bronchial distribution that usually involving upper lobe3,4. CT findings (Figure 3) include central bronchiectasis with mucoid impaction involving predominantly segmental and subsegmental bronchi of the upper lobes and fleeting peripheral air space opacities. In about 30% of patients, the impacted mucus has high density or demonstrates frank calcification at CT scan4.
4. Traction from pulmonary fibrosis
Pulmonary fibrosis in the upper lobes can cause diffuse retraction of the tracheobronchial walls, leading to tracheomegaly. Various kinds of factors such as smoking, chronic bronchitis, emphysema, tuberculosis and sarcoidosis can cause chronic airway inflammation that may result in tracheobronchomalacia. And patients with tracheobronchomalacia present diffuse flaccidity and dilatation of central airway2.
Sarcoidosis is common systemic granulomatous disease of unknown etiology. About 1~3% of patients with sarcoidosis may produce intrinsic granulomatous inflammation of larynx and subglottic trachea or may cause extrinsic compression of airways due to mediastinal lymphadenopathy or extensive mediastinal fibrosis1. Also pulmonary fibrosis caused by sarcoidosis shows cyst formation and traction bronchiectasis in predominantly upper lobe and superior segment of lower lobe3.
Tuberculosis is indolent bacterial infection and often shows relapsing disease course. Pulmonary tuberculosis is usually associated with fibrosis and calcification. In chronic disease, there are fibrosis and scarring with retraction in tracheobronchial trees and also secondary bronchial obstruction can be complicated with fibrosing mediastinitis3.
Diffuse/Multicentric Tracheobronchial Narrowing
1. Tracheobronchomalacia
Tracheobronchomalacia is classified into two subgroups; primary form of the disease is characterized by weakness of the tracheal and central bronchial walls and their supporting structures1. During expiration, central airways show excessive collapse due to increased flaccidity. This form affects mainly children who have congenital cartilage defect. Secondary form of the disease is due to intubation, chronic obstructive airway disease, trauma, recurrent infections, or polychondritis1. This affects older patients who present shortness of breath and wheezing at physical examination1.
CT scan demonstrates tracheal collapse more than 50% in cross-sectional luminal diameter and crescenteric bowing of the posterior membranous trachea ("frown sign") during expiration (Figure 4)5. Dynamic study with paired inspiratory and expiratory CT imaging may help identify abnormal caliber change of the trachea, which may not be noticed on static image1.
2. Infection
1) Tuberculosis with airway involvement
Tuberculosis with airway involvement has been reported in 10~37% of patients with pulmonary parenchymal tuberculosis6. Evaluation of tracheobronchial tuberculosis with CT scan is important to decide extent and management of the disease. CT scan shows irregular or smooth long segmental narrowing with bronchial wall thickening and also extrinsic compression by enlarged tuberculous lymph node. There is often accompanied endoluminal or peribronchial soft tissue masses of low density3. In active stage, the disease usually shows irregular luminal narrowing with bronchial wall thickening (Figure 5A) but, which can be reversible. In fibrotic stage, relatively smooth airway narrowing and minimal wall thickening can be seen (Figure 5B)3.
3. Tracheobronchopathia osteochondroplastica
Tracheobronchopathia osteochondroplastica is rare condition characterized by benign proliferation of bone and cartilage in the tracheal wall3. There are multiple small osteocartilagenous nodules arising from anterolateral tracheal cartilage ring with sparing posterior membranous portion of the trachea1,3. The cause of disease is unknown1. Most patients are male, and the disease usually develops in middle age (5th and 6th decades). The common early symptoms are dyspnea, cough, wheezing, hemoptysis, and recurrent pulmonary infections3. Pathologic finding include foci of submucosal osteocartilaginous growths. The mucosal surface is usually intact, and a connection between the nodule and the perichondrium of the tracheal cartilaginous ring is frequently identified1,3.
4. Diffuse tumor involvement
1) Tracheobronchial papillomatosis
Tracheobronchial papillomatosis is caused by the human papillomavirus (HPV) infection in the upper respiratory tract, usually acquired at birth from an infected mother, however, also can occur in adults2,3. Involvement of the central airways occurs in 5~10% of patients with laryngeal papillomas which is the most common manifestation3. Multifocal infection or aspiration of infected tissue may result in multiple papillary nodules projecting into the airway. Tracheobronchial papillomas are benign disease but are possible carcinomatous transformation to squamous cell carcinoma2.
Radiographic findings include focal or diffuse tracheobronchial nodules or nodular narrowing due to masses arising from mucosal surface of airway (Figure 7). Associated airway obstruction causes atelectasis, air trapping, post-obstructive infection, or bronchiectasis. Disease spread in distal airways produce multiple lung parenchymal nodules, thick-walled cavities or air-filled cysts (pneumatoceles) on CT2,3.
2) Malignant tumor
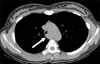
The majority of malignant neoplasm involving central airway is thought to cause focal stenosis. However, sometimes diffuse tumor infiltration is seen and which is either due to primary or secondary malignant tumor. Most common primary tumors of tracheobronchial trees include squamous cell carcinoma and adenoid cystic carcinoma1. Squamous cell carcinoma predominantly occurs in old patients who have the risk factors of cigarette or alcohol abuse7.
Squamous cell carcinoma shows aggressive feature and manifests as large irregular central mass with atelectasis or consolidation on CT scan (Figure 8). Adenoid cystic carcinoma is less aggressive with better prognosis than squamous cell carcinoma7. It usually affects men of 3rd to 5th decades7. CT is valuable to demonstrate primary tumor and its extent. CT scan presents focal polypoid endoluminal masses involving the posterolateral wall of the middle to lower trachea7. Other radiographic findings include total lung atelectasis distal to the tumor and locally aggressive tumor with extraluminal growth (Figure 9)8. Mucoepidermoid carcinoma is the next most common tumor in tracheobronchial trees comprising only about 0.2% of the primary malignancies1,3. This tumor originates from the minor salivary gland lining the tracheobronchial wall. Radiographic findings demonstrate oval or lobulated airway mass which adjust to the branching pattern of the airway. Mucoepidermoid carcinomas usually arise in lobar or segmental bronchus and may have punctate calcification1,3.
Malignancy of central airway from other primary sites may be either due to direct invasion by adjacent tumor or less commonly hematogeneous metastases. The most common malignancies that locally invade the trachea include thyroid, esophagus, larynx and lung3,7. CT scan display asymmetric tracheal narrowing with a soft tissue mass which infiltrates through tracheal cartilages. Hematogenous metastases to tracheal mucosa are rare and mostly arising from breast carcinoma, melanoma, genitourinary malignancies, and sarcoma1,7. CT scan shows single or multiple polypoid soft tissue mass (es) in the lumen of tracheobronchial trees1.
5. Anthracofibrosis
Anthracofibrosis is defined as bronchoscopic finding of bronchostenosis associated with dark anthracotic pigmentation without occupational or environmental exposure to coal dust or smoking9. Clinically, this disease is preponderance in older female patients without association with pneumoconiosis or smoking9. Patients present chronic cough, sputum and dyspnea. Pathological study shows chronic bronchial inflammation with and anthracotic pigmentation9. Pathogenesis is not clear and two hypotheses have been advocated. One is correlation with wood smoke inhalation and the other is correlation with endobronchial tuberculosis9. High prevalence (41~61%) of coexistent active tuberculous infection supports the latter hypothesis9.
6. Saber sheath trachea
Saber sheath trachea is common finding in patients with chronic obstructive pulmonary disease (COPD). It is found when mechanical forces of hyperinflated lungs cause the coronal diameter of the intrathoracic trachea to narrow and the sagittal diameter to elongate so that the sagittal-to-coronal diameter ratio exceeds 2:1 (Figure 11A)2. The extrathoracic trachea remains normal in configuration. CT finding shows side to side narrowing of the trachea at thoracic inlet level (Figure 11B) and mild intrathoracic tracheal wall thickening2.
7. Relapsing polychondritis
Relapsing polychondritis is a rare multisystem autoimmune disorder characterized by recurrent inflammation of the cartilaginous structures of the external ear, nose, peripheral joints, larynx, trachea, and bronchi1,2. The larynx and upper trachea are most commonly involved but the distal airways can be also involved6. The disease also may be accompanied by polyarthritis, aortitis or arteritis and uveal inflammation2. The major airway is involved in greater than 50% of patients and recurrent respiratory infection is the most common cause of morbidity and mortality in these patients1,2.
CT scan demonstrates long segmental narrowing with mural thickening and calcification of the trachea and bronchi characteristically sparing of posterior membranous wall (Figure 12). Cicatricial fibrosis and stenosis of tracheobronchial trees may occur in the late stage1,2. Loss of structural cartilaginous support due to cartilaginous inflammation and destruction may result in excessive compliance and dynamic expiratory collapsibility (tracheomalacia) on fluoroscopy or CT2,6.
8. Amyloidosis
Amyloidosis is systemic condition which is characterized by deposition of fibrillar protein (amyloid) in various organ systems. Pathogenesis is diverse with hereditary, acquired and localized, systemic6. It affects the respiratory tract in approximately 50% of cases3. Amyloid may involve the trachea, bronchi, or more commonly the lung parenchyma1,2,6.
On CT, tracheobronchial involvement of amyloidosis mostly manifests as diffuse nodular and irregular mural thickening and luminal narrowing (Figure 13A), less commonly single or multiple submucosal nodules2. Sometimes, it can accompany lobar or segmental collapse with endobronchial obstruction due to amyloid deposition and component of calcification or ossification3,6. Single or multiple nodules can be seen with pulmonary parenchymal amyloidosis (Figure 13B)6.
9. Wegener's granulomatosis
10. Behcet's disease
Behcet's disease is multisystemic vasculitis of unknown cause that is characterized with various clinical presentations and wide spectrum of thoracic abnormalities3. Pulmonary involvement of Behcet's disease is seen in about 5% of affected patients3. Irregular narrowing resulting from mucosal edema and ulcerative lesions may be seen in trachea and proximal airways6.
11. Extrinsic compression
There are several diseases that induce extrinsic compression of central airways. As a general, mediastinal lymph node diseases, thyroid gland enlargement or mass, mediastinal fibrosis presents various radiographic findings associated with compression of central airways.
1) Lymphadenopathy
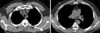
Tuberculous lymphadenitis is the most common cause of lymphadenopathy and is usually a manifestation of primary infection. There is high prevalence in young women, elderly, and immunocompromised patients3. In active stage, CT shows central low density and peripheral rim enhancement of lymph node (Figure 14)3.
Lymphoma with thoracic involvement is classified with Hodgkin's disease (HD) and non-Hodgkin's disease (NHD). About 85% of patients with HD manifest with mediastinal adenopathy3. It shows predilection for the anterior mediastinum and spreading to contiguous nodal groups. Multiple round or bulky matted soft tissue masses are typical finding on contrast-enhanced CT scan. NHD commonly involves paratracheal and anterior mediastinal nodes (Figure 15). About 43% of affected patients can show thoracic involvement at diagnosis.
Castleman's disease (also known as giant lymph node hyperplasia or angiofollicular lymph node hyperplasia) is a form of benign lymphoproliferative disorder of unknown etiology and pathogenesis3. It is classified into two major subgroups of localized disease and multicentric (disseminated) disease. There are two major histologic variants of hyaline vascular and plasma cell types. More than 90% of patients with localized disease have hyaline vascular type and are asymptomatic young adults3. CT findings include a solitary, well-circumscribed hilar or middle posterior mediastinal mass or an infiltrative mass and associated lymphadenopathy with avid uniform contrast enhancement3. Multicentric type is usually plasma cell or mixed type on histology and the patients are often symptomatic older persons.
2) Thyroid enlargement or mass
The normal thyroid gland is usually seen at or just below the level of the cricoid cartilage on CT3. Intrathoracic thyroid masses usually induce displacement or narrowing of the trachea. Benign multinodular goiter is the most common mediastinal mass of thyroid origin. Intrathoracic goiters almost invariably result from downward extension of neck masses into the mediastinum. The mass is heterogeneous and contiguous with the thyroid gland which shows portions of precontrast high attenuation, intense contrast enhancement and coarse calcification3.
3) Fibrosing mediastinitis
Fibrosing (sclerosing) mediastinitis is a rare disorder caused by proliferation of acellular collagen and fibrous tissue within the mediastinum that encases and obstructs vital structures such as SVC, pulmonary arteries and veins, and major airways3. Although many cases are idiopathic, it is usually caused by granulomatous infection, most commonly histoplasmosis (in North America) and tuberculosis. It also may be secondary to exposure to certain drugs, such as methylsergide, and radiation therapy3.
There may be two types of fibrosing mediastinitis, focal and diffuse. The focal type usually manifests as a localized, calcified mass in the paratracheal or subcarinal areas of the mediastinum or in the pulmonary hila, which causes narrowing or occlusion of the adjacent vessels or airways (Figure 16)10. The diffuse type manifests as a diffuse, often noncalcified infiltrative soft tissue mass that obliterates normal mediastinal fat planes and encases or invades adjacent structures. Bronchial narrowing and obstruction is frequently associated with obstructive pneumonitis or atelectasis10.
Conclusion
Awareness of central airway diseases can be increased with thorough radiographic evaluation. Knowledge of radiographic features of diffuse central airway diseases and familiarity with this would help early and proper diagnosis and management. The role of CT with multi-planar and three-dimensional demonstration including virtual bronchoscopy can be emphasized in noninvasive evaluation of central airway diseases.













 XML Download
XML Download