

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Sarcoidosis is a multi-systemic granulomatous disorder of unknown etiology. The characteristic pathological finding is the presence of non-caseating granulomas. The lungs are primarily affected, however other organs may be involved causing various symptoms and ambiguous laboratory findings can be present. There are a few reported cases of sarcoidosis with elevated tumor markers. We describe a 68-year-old woman presenting with sarcoidosis showing elevated serum carcinoembryonic antigen (CEA). The possibility of cancer arising from serum CEA such as gastrointestinal cancer, breast cancer and lung cancer was excluded. A transbronchial lung biopsy demonstrated a non-caseating granuloma without necrosis. As a result prescribed 30 mg prednisolone daily to the patient and serum CEA was decreased after 1 month of treatment. We report a case of pulmonary sarcoidosis with elevated serum CEA.
Figures and Tables

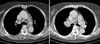
Figure 2
Chest CT scan with enhancement shows enlarged lymph nodes at both hilum, both paratracheal, left paraaotic, AP window and subcarinal nodal station.



References
1. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007. 357:2153–2165.
2. Thuret R, Cariou G, Aerts J, Cochand-Priollet B. Testicular sarcoidosis with elevated levels of cancer-associated markers. J Clin Oncol. 2008. 26:6007–6008.
3. Trimble EL, Saigo PE, Freeberg GW, Rubin SC, Hoskins WJ. Peritoneal sarcoidosis and elevated CA 125. Obstet Gynecol. 1991. 78:976–977.
4. Mulpuru SK, Gujja K, Pai VM, Chen CY, Levey RL. A rare and unusual cause of PSA (prostate-specific antigen) elevation: sarcoidosis of the prostate. Am J Med Sci. 2008. 335:246–248.
5. Furusato B, Koff S, McLeod DG, Sesterhenn IA. Sarcoidosis of the prostate. J Clin Pathol. 2007. 60:325–326.
6. Byun HJ, Won CH, Huh CH, Cho SY, Kim BJ, Kim MN, et al. Clinical observation of sarcoidosis. Korean J Dermatol. 2007. 45:877–883.
7. Hamper UM, Fishman EK, Khouri NF, Johns CJ, Wang KP, Siegelman SS. Typical and atypical CT manifestations of pulmonary sarcoidosis. J Comput Assist Tomogr. 1986. 10:928–936.
8. Judson MA. Sarcoidosis: clinical presentation, diagnosis, and approach to treatment. Am J Med Sci. 2008. 335:26–33.
9. Sekiya K, Sakai T, Homma S, Tojima H. Pulmonary tuberculosis accompanied by a transient increase in serum carcinoembryonic antigen level with tuberculous empyema drainage. Intern Med. 2007. 46:1795–1798.
10. Baughman RP. Pulmonary sarcoidosis. Clin Chest Med. 2004. 25:521–530.
 XML Download
XML Download