

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cavernous sinus syndrome (also called parasellar syndrome) usually presenting with unilateral, progressive painful ophthalmoplegia is caused by disruption of the cranial nerves of the parasellar region. The etiology of cavernous sinus syndrome is difficult to find and diverse including bacterial or fungal infections, non-infectious inflammation, vascular lesions, and neoplasms1. It is relatively rare that metastasis to the parasellar region or cavernous sinus from distant site occur in patients with systemic cancer2,3. In patients with cavernous sinus metastasis, the most common primary sites (sites other than the head and neck) are the breast, prostate, and lung4,5. Herein, we report a case of cavernous sinus metastasis with diagnostic difficulty due to the lack of detectable lesion on brain magnetic resonance imaging (MRI) taken on the time of symptoms.
Case Report
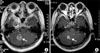
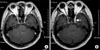
A 50-year-old woman was admitted for evaluation of newly developed ptosis (Figure 1) and headache. She had undergone surgery for lung adenocarcinoma 3 years prior to admission. Her disease was proven to be advanced stage (T4N2M0) because pleural seeding was found during operation. Six cycles of palliative chemotherapy with paclitaxel (175 mg/m2) and cisplatin (60 mg/m2) was given. Right cerebellar metastasis developed almost one year after completion of chemotherapy. Radiotherapy of 3,000 cGy to the whole brain and additional 1,000 cGy to the cerebellum was done. Six months later, she complained of progressive headache and ptosis on the left eye suggestive of third cranial nerve palsy. However, brain MRI showed partial improvement of the previous cerebellar lesion without any newly developed lesions (Figure 2) and repeated CSF studies revealed no abnormalities. We decided to observe her symptoms on an outpatient basis owing to the lack of any diagnostic clue to the cause. Headache and ptosis deteriorated over a period of 6 months. Follow-up MRI revealed a 15×12×7 mm enhancing nodule in the left cavernous sinus which was not detectable on previous brain imaging (Figure 3). After the final diagnosis of cavernous sinus metastasis was made, radiosurgery with cyberknife was done leading to slight improvement of her symptoms. However, leptomeningeal seeding proven by CSF cytology accompanied by drowsy mentality developed 4 months later. Finally, she succumbed to death despite intrathecal chemotherapy and supportive care.
Discussion
Although it is well documented that various types of malignancies metastasize to the parasellar region or cavernous sinus, this metastasis is rarely encountered in clinical practice. Sometimes diagnosis can be challenging, especially when there is no definite abnormality detectable on imaging studies as shown in our case. The rarity of this manifestation in lung cancer patients may also contribute to the difficulty of proper diagnosis.
A pair of intercommunicating venous channels called cavernous sinus is located on either side of the sella turcica. They connect anteriorly to the superior and inferior orbital veins and drain posteriorly into the superior and inferior petrosal sinuses which eventually drain into the sigmoid sinus and internal jugular vein. It is important because of its contents which include the venous plexus, internal carotid artery, periarterial sympathetic nerve fibers, fibrous tissue and cranial nerves III (oculomotor nerve), IV (trochlear nerve), V1 (ophthalmic nerve), V2 (maxillary nerve), and VI (abducens nerve)1. The oculomotor, trochlear, ophthalmic and maxillary nerves are running superoinferiorly in the lateral wall of the cavernous sinus and the abducens nerve passes more medially. Even a small lesion can produce multiple cranial nerve palsies6. Among them, the oculomotor and abducens nerves are most frequently involved, followed by the trochlear nerve7,8. Diplopia, ptosis, ophthalmoplegia, decreased corneal reflex, dysesthesias, hypesthesia, headache, retroorbital pain and facial pain are commonly presenting symptoms3.
Many etiologies such as bacterial or fungal infections, non-infectious inflammation, vascular lesions, and neoplasms is associated with cavernous sinus syndrome1. Among them, tumors in the cavernous sinus area may be primary intracranial neoplasm (e.g., meningioma, pituitary adenoma, craniopharyngioma, sarcoma, chondroma, multiple myeloma, lymphoma), or metastatic tumors, either from close primary tumors (e.g., nasopharyngeal carcinoma, cylindroma) or from distant tumors (breast tumor, prostatic tumor, lung tumor, intestinal tumor, kidney tumor, uterine tumor, testicular tumor, bone tumor, melanoma, indeterminate)2,4,5. Table 1 summarized metastatic diseases from distant site causing cavernous sinus syndrome.
The differential diagnosis of ptosis in lung cancer should include Horner's syndrome, leptomeningeal seeding, cavernous sinus metastasis, trauma, hemorrhage, infection, vasculitis, venovascular hypertension and thrombosis9.
The diagnosis of metastasis to cavernous sinus may be difficult if radiologic finding is lacking10,11. Recently, MRI has become the most useful diagnostic tool when evaluating a suspected cavernous sinus neoplasm12,13. However, in suspected cases, repetition of imaging studies may be necessary because symptoms and signs can precede detectable changes of the cavernous sinus on diagnostic imaging10,13,14. The necessity of biopsy is unclear, especially in patients with known systemic cancer with image-confirmed cavernous sinus lesions15.
The management of cavernous sinus metastasis is palliative5,15. Generally, radiation therapy is performed as standard treatment and often leads to improvement of symptoms and alleviation of pain13. However, the prognosis is very poor and the median survival is reported to be 4~4.5 months from the onset of symptoms3,5. Therefore, lack of radiologic abnormalities should not be taken as evidence for the absence of metastatic lesions and treatment should be started under a clinical diagnosis because local treatment such as radiotherapy may relieve or alleviate the symptoms completely11,16.
When a strong clinical suspicion of cavernous sinus metastasis exists, thorough neurologic examination and serial brain imaging should be followed up to avoid overlooking the lesion and treatment should be started immediately under a clinical diagnosis.


 XML Download
XML Download