

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hyun Kuk Kim, M.D.1, Eun Young Choi, M.D.2, Jae Seung Lee, M.D.2, Yun Jeong Bae, M.D.3, Jin Woo Song, M.D.2, 4, Tae-Bum Kim, M.D.3, 4, You Sook Cho, M.D.3, 4 , Hee-Bom Moon, M.D.3, 4, Sang Do Lee, M.D.2, 4, Yeon-Mok Oh, M.D.2, 4
, Hee-Bom Moon, M.D.3, 4, Sang Do Lee, M.D.2, 4, Yeon-Mok Oh, M.D.2, 4
, Hee-Bom Moon, M.D.3, 4, Sang Do Lee, M.D.2, 4, Yeon-Mok Oh, M.D.2, 4
Abstract
Background
Rhinolaryngoscopy and sputum examination are popular tests for the evaluation of chronic cough. Little is known about the relationship between symptoms and rhinolaryngoscopic findings or sputum eosinophilia in chronic cough patients.
Methods
One hundred patients, who had chronic cough with normal chest radiography and who also had undergone both rhinolaryngoscopy and induced sputum analysis, were reviewed retrospectively. Eleven associated symptoms of chronic cough were asked; postnasal drip (PND) and laryngopharyngeal reflux (LPR) were examined by rhinolaryngoscopy. Induced sputum analysis was performed for evaluation of sputum eosinophilia. Cross tabulation analyses with chi-square tests were used to evaluate the relationship between symptoms and objective findings.
Results
The most frequent symptom was sputum (70%). The prevalence of PND and LPR on rhinolaryngoscopy were 56% (56/100) and 25.6% (22/86), respectively. Sputum eosinophilia was observed in 23 (23.7%) of 97 patients. The dyspnea (p=0.001), sputum (p=0.003), nasal obstruction (p=0.023), and postnasal drip sense (p=0.025) were related with PND on rhinolaryngoscopy. LPR on rhinolaryngoscopy was not related with any symptoms. Dyspnea (p=0.003), wheezing (p=0.005), nasal obstruction (p=0.013), and belching (p=0.018) were related with sputum eosinophilia.
Figures and Tables
Figure 1
Endoscopes for the evaluation of nasal cavity, pharynx and larynx. The upper endoscope has 70° angle at the tip and was used to examine the oropharynx and larynx. The lower one was used to examine the inside of the nasal cavity and nasopharyngeal mucosa.

Figure 2
Percentage of patients with each symptom among all of the chronic cough patients. PND: postnasal drip.
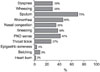
Figure 3
Percentage of patients with positive findings in rhinolaryngoscopy and induced sputum among all of the chronic cough patients. PND: postnasal drip on rhinolaryngoscopy; LPR: laryngopharyngeal reflux on rhinolaryngoscopy.

Figure 4
The comparison of frequency of symptoms according as whether postnasal drip (PND) existed on rhinolaryngoscopy. *p-value <0.05, †p-value <0.01.

Figure 5
The comparison of frequency of symptoms between laryngopharyngeal reflux (LPR) negative and LPR positive patients on rhinolaryngoscopy. PND: postnasal drip.

Figure 6
The comparison of frequency of symptoms depending on the existence of sputum eosinophilia. PND: postnasal drip. *p-value <0.05, †p-value <0.01.



Acknowledgements
This study was supported by a grant of the Korea Healthcare technology R&D Project, Ministry for Health, Welfare and Family Affairs, Republic of Korea (A040153).
References
1. Irwin RS, Madison JM. The diagnosis and treatment of cough. N Engl J Med. 2000. 343:1715–1721.
2. Pratter MR. Chronic upper airway cough syndrome secondary to rhinosinus diseases (previously referred to as postnasal drip syndrome): ACCP evidence-based clinical practice guidelines. Chest. 2006. 129:1 Suppl. 63S–71S.
3. Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology-Head and Neck Surgery. Otolaryngol Head Neck Surg. 2002. 127:32–35.
4. Belafsky PC, Postma GN, Koufman JA. The validity and reliability of the reflux finding score (RFS). Laryngoscope. 2001. 111:1313–1317.
5. Belafsky PC, Postma GN, Koufman JA. Validity and reliability of the reflux symptom index (RSI). J Voice. 2002. 16:274–277.
6. Sohn SW, Yang MS, Lee SH, Song WJ, Lee SM, Kwon HS, et al. Evaluation of the causes of chronic cough with sputum eosinophilia. Korean J Asthma Allergy Clin Immunol. 2007. 27:125–130.
7. Kwon NH, Oh MJ, Min TH, Lee BJ, Choi DC. Causes and clinical features of subacute cough. Chest. 2006. 129:1142–1147.
8. Mello CJ, Irwin RS, Curley FJ. Predictive values of the character, timing, and complications of chronic cough in diagnosing its cause. Arch Intern Med. 1996. 156:997–1003.
9. McGarvey LP, Heaney LG, Lawson JT, Johnston BT, Scally CM, Ennis M, et al. Evaluation and outcome of patients with chronic non-productive cough using a comprehensive diagnostic protocol. Thorax. 1998. 53:738–743.
10. Stankiewicz JA, Chow JM. Nasal endoscopy and the definition and diagnosis of chronic rhinosinusitis. Otolaryngol Head Neck Surg. 2002. 126:623–627.
11. Ylitalo R, Lindestad PA, Ramel S. Symptoms, laryngeal findings, and 24-hour pH monitoring in patients with suspected gastroesophago-pharyngeal reflux. Laryngoscope. 2001. 111:1735–1741.
12. Brightling CE, Ward R, Goh KL, Wardlaw AJ, Pavord ID. Eosinophilic bronchitis is an important cause of chronic cough. Am J Respir Crit Care Med. 1999. 160:406–410.
13. Wark PA, Gibson PG, Fakes K. Induced sputum eosinophils in the assessment of asthma and chronic cough. Respirology. 2000. 5:51–57.
14. Pratter MR, Bartter T, Akers S, DuBois J. An algorithmic approach to chronic cough. Ann Intern Med. 1993. 119:977–983.
15. Selner JC. Visualization techniques in the nasal airway: their role in the diagnosis of upper airway disease and measurement of therapeutic response. J Allergy Clin Immunol. 1988. 82:909–916.
 XML Download
XML Download