

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
The global number of Mycobacterium avium complex (MAC) pulmonary infection is increasing. Patients with preexisting lung disease or who are immunodeficient are at the greatest risk for developing MAC infection. Endobronchial lesions with MAC infection are rare in the immunocompetent host. However, there have been an increasing number of reports of an immunocompetent host being afflicted with various manifestations of MAC infection. We report a case of pulmonary and endobronchial MAC infection presenting as an acute pneumonia in a 59-year-old female without preexisting lung disease or immunodeficiency.
Figures and Tables
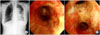
Figure 1
Initial chest X-ray shows infiltrations with nodular densities in left middle and left lower lung (A). Chest CT scan shows left pleural effusion, multifocal consolidation and nodular lesion with cavitation in left lung field (B).

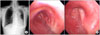
Figure 2
After 10 days of admission, aggravated infiltration of left lung is noted in chest radiograph (A) and bronchoscopy shows hyperemic irregular mucosal lesion in left main bronchus and left upper lobar bronchus (B).
References
1. Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007. 175:367–416.
2. Medical Section of the American Lung Association. Diagnosis and treatment of disease caused by nontuberculous mycobacteria. This official statement of the American Thoracic Society was approved by the Board of Directors, March 1997. Am J Respir Crit Care Med. 1997. 156:S1–S25.
3. Waller EA, Roy A, Brumble L, Khoor A, Johnson MM, Garland JL. The expanding spectrum of Mycobacterium avium complex-associated pulmonary disease. Chest. 2006. 130:1234–1241.
4. Lee JH, Son KS, Park JH, Kim JC, Lee HW, Kim CH. Mycobacterium avium infection presenting as endobronchial lesions in an immunocompetent patient. Tuberc Respir Dis. 2006. 60:571–575.
5. Bak JY, Kim KS, Park IN, Yum HK, Lee SH, Lee HK, et al. Two cases of hot tub lung in bodyscrubbers working in a public bath. Tuberc Respir Dis. 2009. 66:37–41.
6. Shih JY, Wang HC, Chiang IP, Yang PC, Luh KT. Endobronchial lesions in a non-AIDS patient with disseminated Mycobacterium avium-intracellulare infection. Eur Respir J. 1997. 10:497–499.
7. Kim SS, Rhie EJ, Ko GJ, Choi HS, Oh HE, Kim JM, et al. A case of mycobacterium avium pulmonary disease with massive pleural effusion in an HIV-negative, nonimmunosuppressed patient: using PCR-restriction fragment length polymorphism assay. Infect Chemother. 2004. 36:381–385.
8. Litman DA, Shah UK, Pawel BR. Isolated endobronchial atypical mycobacterium in a child: a case report and review of the literature. Int J Pediatr Otorhinolaryngol. 2000. 55:65–68.
9. Fukuoka K, Nakano Y, Nakajima A, Hontsu S, Kimura H. Endobronchial lesions involved in Mycobacterium avium infection. Respir Med. 2003. 97:1261–1264.
10. Chung HS, Lee JH. Bronchoscopic assessment of the evolution of endobronchial tuberculosis. Chest. 2000. 117:385–392.
11. Garay SM. Rom WN, Garay SM, editors. Pulmonary tuberculosis. Tuberculosis. 2004. 2nd ed. Philadelphia: Lippincott Williams & Wilkins;345–394.
12. Iseman MD. Medical management of pulmonary disease caused by Mycobacterium avium complex. Clin Chest Med. 2002. 23:633–641.
 XML Download
XML Download