

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Recently, many institutions have acquired multi-detector computed tomography (MDCT) systems. This made it easier and more convenient to use MDCT as a initial diagnostic modality for hemoptysis. The purpose of this study was to evaluate the usefulness of MDCT before bronchoscopy and/or bronchial arterial embolization (BAE) for hemoptysis.
Methods
We studied a total of 125 patients with hemoptysis who underwent, between 2006 and 2008, MDCT in a routine protocol before bronchoscopy and/or BAE. One hundred two patients underwent bronchoscopy and 29 patients underwent BAE. We compared the usefulness of MDCT and bronchoscopy for detecting the bleeding site and identifying the cause. We also evaluated our ability, using MDCT, to detect instances where the bronchial artery caused hemoptysis.
Results
The rate of detection of a bleeding site was 75.5% on MDCT and 50.9% on bronchoscopy. MDCT and bronchoscopy detected the bleeding site in agreement in 62.7% of patients. MDCT alone found the bleeding site in 27.5% of cases. MDCT identified the cause of hemoptysis in 77.5% and bronchoscopy in 11.8%. In 29 patients who underwent BAE, we detected a total of 37 hypertrophied bronchial arteries that were causing hemoptysis. Of 37 bronchial arteries, 23 (62.2%) were depicted on MDCT.
Conclusion
MDCT is superior to bronchoscopy for detecting the bleeding site and identifying the cause of hemoptysis. MDCT can also predict the side of affected bronchial artery with depiction of hypertrophied bronchial artery and localizing the bleeding site. Doing MDCT before bronchoscopy and BAE can provide a guideline for the next step.
Figures and Tables
Figure 1
Endobronchial metastasis from renal cell carcinoma in a 59-year-old man with non-massive hemoptysis. (A) Axial multi-detector computed tomography scans show well-enhanced endobronchial nodule with bronchial obstruction in posterobasal segment of right lower lobe. (B) On bronchoscopic examination, polypoid nodule with bleeding at orifice of posterobasal segmental bronchus of right lower lobe was identified.
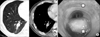
Figure 2
Bronchiectasis in a 47-year-old woman with massive hemoptysis. (A) Axial multi-detector computed tomography (MDCT) scans show ground-glass opacity with bronchiectasis in left lower lobe and a hypertrophied left bronchial artery (arrow). (B, C) Coronal reconstructed MDCT scan and selective left bronchial angiogram show a hypertrophied left bronchial artery (arrows). On bronchoscopic examination, active bleeding from left lower lobe bronchial tree was identified.

Figure 3
Active pulmonary tuberculosis in a 37-year-old man with non-massive hemoptysis. (A) Axial multi-detector computed tomography (MDCT) scan shows ground-glass opacity in apical segment of right upper lobe. No detectable hypertrophied bronchial artery on MDCT scan. (B) Selective right bronchial angiogram shows a minimally dilated right bronchial artery (arrow) with hypervascular tissue staining (arrowhead) in right upper lung zone.





References
1. Jean-Baptiste E. Clinical assessment and management of massive hemoptysis. Crit Care Med. 2000. 28:1642–1647.
2. Sirajuddin A, Mohammed TL. A 44-year-old man with hemoptysis: a review of pertinent imaging studies and radiographic interventions. Cleve Clin J Med. 2008. 75:601–607.
3. Tsoumakidou M, Chrysofakis G, Tsiligianni I, Maltezakis G, Siafakas NM, Tzanakis N. A prospective analysis of 184 hemoptysis cases: diagnostic impact of chest X-ray, computed tomography, bronchoscopy. Respiration. 2006. 73:808–814.
4. Bidwell JL, Pachner RW. Hemoptysis: diagnosis and management. Am Fam Physician. 2005. 72:1253–1260.
5. Khalil A, Soussan M, Mangiapan G, Fartoukh M, Parrot A, Carette MF. Utility of high-resolution chest CT scan in the emergency management of haemoptysis in the intensive care unit: severity, localization and aetiology. Br J Radiol. 2007. 80:21–25.
6. Hsiao EI, Kirsch CM, Kagawa FT, Wehner JH, Jensen WA, Baxter RB. Utility of fiberoptic bronchoscopy before bronchial artery embolization for massive hemoptysis. AJR Am J Roentgenol. 2001. 177:861–867.
7. Revel MP, Fournier LS, Hennebicque AS, Cuenod CA, Meyer G, Reynaud P, et al. Can CT replace bronchoscopy in the detection of the site and cause of bleeding in patients with large or massive hemoptysis? AJR Am J Roentgenol. 2002. 179:1217–1224.
8. Yoon YC, Lee KS, Jeong YJ, Shin SW, Chung MJ, Kwon OJ. Hemoptysis: bronchial and nonbronchial systemic arteries at 16-detector row CT. Radiology. 2005. 234:292–298.
9. Khalil A, Fartoukh M, Tassart M, Parrot A, Marsault C, Carette MF. Role of MDCT in identification of the bleeding site and the vessels causing hemoptysis. AJR Am J Roentgenol. 2007. 188:117–125.
10. Chung MJ, Lee JH, Lee KS, Yoon YC, Kwon OJ, Kim TS. Bronchial and nonbronchial systemic arteries in patients with hemoptysis: depiction on MDCT angiography. AJR Am J Roentgenol. 2006. 186:649–655.
11. Bruzzi JF, Remy-Jardin M, Delhaye D, Teisseire A, Khalil C, Remy J. Multi-detector row CT of hemoptysis. Radiographics. 2006. 26:3–22.
12. Remy-Jardin M, Bouaziz N, Dumont P, Brillet PY, Bruzzi J, Remy J. Bronchial and nonbronchial systemic arteries at multi-detector row CT angiography: comparison with conventional angiography. Radiology. 2004. 233:741–749.
13. Rémy J, Voisin C, Dupuis C, Beguery P, Tonnel AB, Denies JL, et al. Treatment of hemoptysis by embolization of the systemic circulation. Ann Radiol (Paris). 1974. 17:5–16.
14. Unsal E, Koksal D, Cimen F, Taci Hoca N, Sipit T. Analysis of patients with hemoptysis in a reference hospital for chest diseases. Tuberk Toraks. 2006. 54:34–42.
15. Eisenhuber E, Brunner C, Bankier AA. Blood clots mimicking peripheral intrabronchial tumors in patients with hemoptysis: CT and bronchoscopic findings. J Comput Assist Tomogr. 2000. 24:47–51.
16. Ekim H, Sanisoglu I, Akar H. Hemoptysis: bronchoscopic-computed tomographic correlation in ninety eight cases. Eastern J Med. 2000. 5:21–25.
 XML Download
XML Download