

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
In previous study, most patients with bronchial anthracofibrosis (BAF) were non-miners, and non-occupational old aged females. However, the clinical significance of BAF in patients with coal workers' pneumoconiosis (CWP) is unknown.
Methods
Among patients with CWP who transferred to our hospital for an evaluation of associated pulmonary diseases, 32 patients who had undergone a bronchofibroscopy (BFS) and chest computed tomography (CT) examination were evaluated for the association of the BAF using a retrospective chart review.
Results
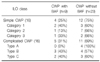
Nine of the 32 CWP patients (28%) were complicated with BAF. Four of the 16 simple CWP patients (25%) were complicated with BAF. According to the International Labor Organization (ILO) classification by profusion, 2 out of 3 patients in category 1, 1 out of 8 patients in category 2 and 1 out of 3 patients in category 3 were complicated with BAF. Five out of 16 complicated CWP patients were complicated with BAF. Three out of 7 patients in type A and 2 out of 5 patients in type C were complicated with BAF. CWP patients with BAF had significantly greater multiple bronchial thickening and multiple mediastinal or hilar lymph node enlargement than the CWP patients without BAF. There was no difference in the other clinical features between the CWP patients with BAF and those without BAF.
Conclusion
Many CWP patients were complicated with BAF. The occurrence of BAF was not associated with the severity of CWP progression. Therefore, a careful evaluation of the airway with a bronchoscopy examination and chest CT is warranted for BAF complicated CWP patients who present with respiratory symptoms and signs, even ILO class category 1 simple CWP patients.
Figures and Tables
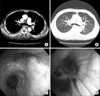 | Figure 170-year-old man with coal workers' pneumoconiosis associated with bronchial anthracofibrosis. (A) Contrast enhanced CT shows bronchial wall thickening due to enlarged lymph node and peribronchial fibrosis. (B) Lung setting on CT shows multiple p type nodules in the both upper lobes. (C) Flexible bronchoscopy shows bronchial narrowing with engorged mucosal vessel and anthracotic pigmentation in the right upper lobe bronchus. (D) Anthracotic pigmentation and bronchial stenosis is also noted in the right middle lobe bronchus.
|

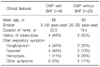
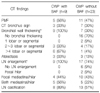
Table 2
The difference of clinical characteristics between coal workers' pneumoconiosis with and without bronchial anthracofibrosis
![]()
References
1. Jang SJ, Lee SY, Kim SC, Lee SY, Cho HS, Park KH, et al. Clinical and radiological characteristics of non-tuberculous bronchial anthracofibrosis. Tuberc Respir Dis. 2007. 63:139–144.
2. Lee HS, Maeng JH, Park PG, Jang JG, Park W, Ryu DS, et al. Clinical features of simple bronchial anthracofibrosis which is not associated with tuberculosis. Tuberc Respir Dis. 2002. 53:510–518.
3. Ryder RC, Lyons JP, Campbell H, Gough J. Bronchial mucous gland status in coal workers' pneumoconiosis. Ann N Y Acad Sci. 1972. 200:370–380.
4. Chong S, Lee KS, Chung MJ, Han J, Kwon OJ, Kim TS. Pneumoconiosis: comparison of imaging and pathologic findings. Radiographics. 2006. 26:59–77.
5. Remy-Jardin M, Remy J, Farre I, Marquette CH. Computed tomographic evaluation of silicosis and coal workers' pneumoconiosis. Radiol Clin North Am. 1992. 30:1155–1176.
6. Voisin C, Macquet L, Lenoir L, Houcke M, Savinel E, Muchery-Piat G. Bronchial involvement in diverse stages of pneumoconiosis in coal miners. Bronches. 1965. 15:449–461.
7. Mulliez P, Billon-Galland MA, Dansin E, Janson X, Plisson JP. Bronchial anthracosis and pulmonary mica overload. Rev Mal Respir. 2003. 20(2 Pt 1):267–271.
8. Huttner H, Beyer M, Bargon J. Charcoal smoke causes bronchial anthracosis and COPD. Med Klin (Munich). 2007. 102:59–63.
9. International Labour Office. International classification of radiographs of pneumoconiosis. 2001. 1st ed. Geneva: International Labour Office.
10. Ryu DS, Jung SM, Lee DH, Kim NH, Jung BH, Chung HR, et al. CT and MR findings of bronchial anthracofibrosis. J Korean Radiol Soc. 2000. 42:481–486.
11. Choi BS. Development of coalworkers' pneumoconiosis in Korea: risk factors and incidence density. Korean J Occup Environ Med. 1996. 8:137–152.
12. Churg A, Brauer M. Human lung parenchyma retains PM2.5. Am J Respir Crit Care Med. 1997. 155:2109–2111.
13. No TM, Kim IS, Kim SW, Park DH, Joeng JK, Ju DW, et al. The clinical investigation for determining the etiology of bronchial anthracofibrosis. Korean J Med. 2003. 65:665–674.
14. Kim YJ, Jung CY, Shin HW, Lee BK. Biomass smoke induced bronchial anthracofibrosis: presenting features and clinical course. Respir Med. 2009. 103:757–765.
15. Bircan HA, Bircan S, Ozturk O, Ozyurt S, Sahin U, Akkaya A. Mediastinal tuberculous lymphadenitis with anthracosis as a cause of vocal cord paralysis. Tuberk Toraks. 2007. 55:409–413.
16. Kim SW, Kim IS, Park DH, No TM, Joeng JK, Jung SW, et al. The clinical significances of bronchial anthracofibrosis in the patients with endobronchial tuberculosis. Tuberc Respir Dis. 2004. 56:495–504.
17. Cohen RA, Patel A, Green FH. Lung disease caused by exposure to coal mine and silica dust. Semin Respir Crit Care Med. 2008. 29:651–661.
18. Shin PJ, Yong SJ, Shin KC, Lee WY, Kim ST, Cha BS, et al. Clinical significance of serum PDGF-BB and IGF-1 in coal workers' pneumoconiosis. Tuberc Respir Dis. 2002. 52:338–345.
19. Lee JY, Yoo KH, Ahn HR, Kim SR, Lee HW, Ahn CM, et al. The role of lymphocyte compartment and cytokine in coal workers pneumoconiosis. Tuberc Respir Dis. 2002. 52:241–250.
20. Paterson BF, Patterson R, Grammer LC. Pathogenesis of occupational lung disease. Clin Rev Allergy. 1986. 4:303–321.
21. Bergin CJ, Muller NL, Vedal S, Chan-Yeung M. CT in silicosis: correlation with plain films and pulmonary function tests. AJR Am J Roentgenol. 1986. 146:477–483.
 XML Download
XML Download