

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Seo Woo Kim, M.D.1, Hyun Kyung Kim, M.D.1, Sung Joung Jeun, M.D.1, Hye Sung Park, M.D.1, Jung Hyun Jang, M.D.1, Jin Hwa Lee, M.D.1 , Yon Ju Ryu, M.D.1, Sung Shin Sim, M.D.2, Eun Mi Chun, M.D.1
, Yon Ju Ryu, M.D.1, Sung Shin Sim, M.D.2, Eun Mi Chun, M.D.1
, Yon Ju Ryu, M.D.1, Sung Shin Sim, M.D.2, Eun Mi Chun, M.D.1
Abstract
Lymphadenopathy in the thoracic cavity is frequently caused by inflammatory diseases. In very rare cases, the node-bronchial fistula has been reported to be the cause of complications of pulmonary tuberculosis. A male patient with necrotizing pneumonia and mediastinal lymph node enlargements identified by chest computed tomography was also found to have a node-bronchial fistula caused by lung cancer. The patient was treated for tuberculosis with pneumonia for one week before a definitive diagnosis was made. A further investigation revealed him to have non-small cell lung cancer (NSCLC, adenocarcinoma) and multiple mediastinal lymphadenopathies accompanied with the node-bronchial fistula. We report this specific case that had been previously treated for tuberculosis but was later revealed to be NSCLC accompanied with a node-bronchial fistula.
Figures and Tables
 | Figure 1Chest X-ray on admission showed multiple consolidations in right upper lung zone and left lingular lobe.
|
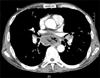 | Figure 2Chest CT scan revealed subcarinal lymph node enlargement with air bubbles (possible node-bronchial fistula between airway and subcarinal lymph node). Multiple necrotic lymph nodes enlargement were seen in mediastium, both hilar, retrosternal and lower cervical area.
|


References
1. Im JG, Lee KS. The chest radiology. 2000. 1st ed. Seoul: Ilchokak.
2. Iselin H, Suter F. The role of perforation of hilar lymph nodes into the bronchial tree of adults. Chest. 1954. 25:302–311.
3. Jiang B, Wu GP, Zhao YJ, Wang SC. Transcription expression and clinical significance of TTF-1 mRNA in pleural effusion of patients with lung cancer. Diagn Cytopathol. 2008. 36:849–854.
4. Mountain CF, Dresler CM. Regional lymph node classification for lung cancer staging. Chest. 1997. 111:1718–1723.
5. Lois M, Noppen M. Bronchopleural fistulas: an overview of the problem with special focus on endoscopic management. Chest. 2005. 128:3955–3965.
6. Park EH, Jang TW, Park MI, Song JY, Choi IS, Oak CH, et al. A case of esophago-mediatinal fistula due to esophageal tuberculosis. Tuberc Respir Dis. 2007. 62:531–535.
7. Gu P, Zhao YZ, Jiang LY, Zhang W, Xin Y, Han BH. Endobronchial ultrasound-guided transbronchial needle aspiration for staging of lung cancer: a systematic review and meta-analysis. Eur J Cancer. 2009. 45:1389–1396.
8. Zwischenberger JB, Savage C, Alpard SK, Anderson CM, Marroquin S, Goodacre BW. Mediastinal transthoracic needle and core lymph node biopsy: should it replace mediastinoscopy? Chest. 2002. 121:1165–1170.
9. Wang MZ, Wan XB, Chen Y, Zhang L, Zhong W, Zhong X, et al. The results of transbronchial needle aspiration in 164 cases with enlarged mediastinal and/or hilar lymph nodes. Zhonghua Nei Ke Za Zhi. 2009. 48:133–135.
10. Fritscher-Ravens A, Bohuslavizki KH, Brandt L, Bobrowski C, Lund C, Knofel WT, et al. Mediastinal lymph node involvement in potentially resectable lung cancer: comparison of CT, positron emission tomography, and endoscopic ultrasonography with and without fine-needle aspiration. Chest. 2003. 123:442–451.
 XML Download
XML Download