

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hae-Seong Nam, M.D.1, Dong-Hyuk Yang, M.D.1, Jeong-Soo Kim, M.D.1, Hyun-Jung Kim, R.N.1, Hyeon Gyu Yi, M.D.2, Kyung Hee Lee, M.D.3, Jae Hwa Cho, M.D.1 , Yong Han Yoon, M.D.4, Seung Min Kwak, M.D.1, Hong Lyeol Lee, M.D.1, Kwang Ho Kim, M.D.4, Jeong-Seon Ryu, M.D.1
, Yong Han Yoon, M.D.4, Seung Min Kwak, M.D.1, Hong Lyeol Lee, M.D.1, Kwang Ho Kim, M.D.4, Jeong-Seon Ryu, M.D.1
, Yong Han Yoon, M.D.4, Seung Min Kwak, M.D.1, Hong Lyeol Lee, M.D.1, Kwang Ho Kim, M.D.4, Jeong-Seon Ryu, M.D.1
Abstract
Slowly growing lung cancers are quite rare and the leading cause of length time bias and over-diagnosis bias in lung cancer screening. We report 6 cases of slowly growing lung cancer in a tertiary hospital between January 1999 and December 2008. The clinical characteristics of these 6 cases with slowly growing lung cancer were examined. The median age at diagnosis was 68 years (range, 49~72), and 5 patients (83%) were female. The most common histology type was adenocarcinoma (83%). After excluding two patients who showed no change in the tumor size, the median tumor doubling time was 189 months (range, 86~387). The proportion of patients with slowly growing lung cancer appears to be particularly large in women, especially among patients with adenocarcinoma. Our experience shows that slowly growly lung cancers are more heterogeneous and diverse.
Figures and Tables
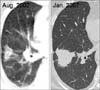
 | Figure 1Transverse CT scans obtained 40 months apart in patient 1 show no growth in nodule of right upper lobe (RLU). However, area of sold attenuation is increased. This nodule was confirmed to adenocarcinoma by RUL obectomy.
|
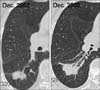
 | Figure 2Transverse CT scans obtained 53 months apart in patient 4 (tumor doubling time, 142 months) show increase in size (2.6 → 3.8 cm) of mass in right lower lobe. Area of sold attenuation is also increased. This mass was confirmed to adenocarcinoma by sputum cytology.
|

References
1. Molina JR, Adjei AA, Jett JR. Advances in chemotherapy of non-small cell lung cancer. Chest. 2006. 130:1211–1219.
2. Patz EF Jr, Goodman PC, Bepler G. Screening for lung cancer. N Engl J Med. 2000. 343:1627–1633.
3. Jeong HC, Lee SY, Oh YH, In KH, Kim HG, Yoo SH. An adenocarcinoma of lung with unusual very slow growth: a case report. J Lung Cancer. 2006. 5:51–54.
4. Kwon KD, Kim JH, Kim DY, Choi MH, Choi JH, Shin DW, et al. A case of adenocarcinoma presenting a solitary pulmonary nodule that grows slowly over 10 years. Tuberc Respir Dis. 2008. 64:318–323.
5. Yoon BK, Kim EJ, Kim DI, Lee KH, Ryu JS, Kwak SM, et al. A case of adenocarcinoma presenting a solitary pulmonary nodule that showed no growth over 4 years. Tuberc Respir Dis. 2005. 59:326–329.
6. Detterbeck FC, Gibson CJ. Turning gray: the natural history of lung cancer over time. J Thorac Oncol. 2008. 3:781–792.
7. Hasegawa M, Sone S, Takashima S, Li F, Yang ZG, Maruyama Y, et al. Growth rate of small lung cancers detected on mass CT screening. Br J Radiol. 2000. 73:1252–1259.
8. Lindell RM, Hartman TE, Swensen SJ, Jett JR, Midthun DE, Tazelaar HD, et al. Five-year lung cancer screening experience: CT appearance, growth rate, location, and histologic features of 61 lung cancers. Radiology. 2007. 242:555–562.
9. Hillerdal G. Indolent lung cancers: time for a paradigm shift: a review. J Thorac Oncol. 2008. 3:208–211.
10. Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007. 2:706–714.
11. Joseph WL, Morton DL, Adkins PC. Prognostic significance of tumor doubling time in evaluating operability in pulmonary metastatic disease. J Thorac Cardiovasc Surg. 1971. 61:23–32.
12. Aoki T, Nakata H, Watanabe H, Nakamura K, Kasai T, Hashimoto H, et al. Evolution of peripheral lung adenocarcinomas: CT findings correlated with histology and tumor doubling time. AJR Am J Roentgenol. 2000. 174:763–768.
13. Marcus PM, Bergstralh EJ, Fagerstrom RM, Williams DE, Fontana R, Taylor WF, et al. Lung cancer mortality in the Mayo Lung Project: impact of extended follow-up. J Natl Cancer Inst. 2000. 92:1308–1316.
14. Bach PB, Jett JR, Pastorino U, Tockman MS, Swensen SJ, Begg CB. Computed tomography screening and lung cancer outcomes. JAMA. 2007. 297:953–961.
15. Bepler G, Goodridge Carney D, Djulbegovic B, Clark RA, Tockman M. A systematic review and lessons learned from early lung cancer detection trials using low-dose computed tomography of the chest. Cancer Control. 2003. 10:306–314.
 XML Download
XML Download