

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
A benign metastasizing leiomyoma (BML) is a rare condition that is characterized by the benign histological appearance and presence of well-differentiated smooth muscle cells in the lesions. This condition may present in women of any age with uterine leiomyoma. The patients are usually asymptomatic with the pulmonary lesions generally being discovered incidentally. The lung is the most common site of involvement1,2.
We report two cases of a benign metastasizing leiomyoma in women with a history of uterine leiomyoma.
Case Report
Case 1
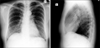
A 35-year-old woman presented after the initial radiology evaluation incidentally revealed the presence of multiple lung nodules. She complained of cough and whitish sputum but she denied dyspnea, hemoptysis or fever. There was no history of malignancy. Her medical history included only myomectomy and a cesarean section performed approximately 6 years earlier. No abnormal sounds were present upon auscultation of the chest. A chest X-ray revealed two lung nodules (Figure 1). A chest CT was subsequently performed, which demonstrated two nodules, one 0.8 cm diameter nodule in the right middle lobe and the another 1.0 cm diameter nodule in the left upper lobe (Figure 2). There was no mediastinal lymphadenopathy. A diagnostic transthoracic needle biopsy was performed and she was finally diagnosed with a benign metastasizing leiomyoma (Figure 3). The patient then received LH-RH and has been followed up since.
Case 2
A 44-year-old woman presented after an initial radiology evaluation incidentally revealed the presence of multiple, small-sized lung nodules. The patient denied dyspnea, cough, sputum production, hemoptysis or fever and there was no history of a malignancy. Her significant medical history included only a total hysterectomy performed approximately 10 years earlier. No crackles nor rales were present upon auscultation of the chest. A chest X-ray showed multiple lung nodules (Figure 4). CT of the chest was subsequently performed, which demonstrated multiple lung nodules ranging in size from a few millimeters to 2 cm in diameter (Figure 5). However, there was no mediastinal lymphadenopathy, pleural effusion or calcification. A diagnostic percutaneous biopsy was performed. The lesions were mainly suspected of being a benign spindle cell tumor. She underwent a right middle lung wedge resection to confirm the diagnosis and was finally diagnosed with a benign metastasizing leiomyoma (Figure 6). The patient did not receive any further treatment, and the multiple lung nodules have been followed up closely.
Discussion
Leiomyomas are the most common benign uterine neoplasms of the myometrium. However, a BML is a rare condition characterized by the occurrence of benign smooth muscle tumors. These lesions are most often located in the lung in association with uterine leiomyomatosis. Other sites of involvement include the pelvic lymph nodes, skull base, spine, brain, heart, ret roperitoneum etc1,2. This condition may present in women of any age with uterine leiomyoma. Abramson et al3 reported that nodules can be observed 3 months to 20 years after a hysterectomy or myomectomy. The clinical course is typically indolent, with the patient mortality commonly occurring from an unrelated disease process. There is little correlation between the extent of the disease and the respiratory symptoms3.
The etiology of metastasizing leiomyomas includes the presence of metastatic disease from an existing leiomyoma and the presence of multicentric leiomyomatous growths4-6. Estrogen and progesterone receptors have been identified on the lung lesions, which has led to treatment options based on hormonal therapy through surgery or medical oophorectomy. However, surgery or hormonal therapy may not always be indicated. The effects of natural hormonal changes such as pregnancy and menopause have also been associated with the regression of these lesions7.
Almost all patients reported thus far were Caucasians. We report two Oriental patients. One woman had myomectomy performed before the discovery of her pulmonary lesions, and the other underwent a total hysterectomy and myomectomy. Both experienced surgical trauma such as a hysterectomy or myomectomy. These cases further support the higher risk of a benign metastasizing leiomyoma after a surgical procedure on the uterus. In our cases, one woman was closely observed without any management for 5 years. Despite the numerous lung nodules, she has rarely complained of respiratory symptoms such as dyspnea, cough, sputum production and hemoptysis. She has remained stable without any evidence of aggravation.
To our knowledge, there are only 2 other cases reported in Korea. Both underwent a hysterectomy due to a benign uterine leiomyoma. After being diagnosed with abenign metastasizing leiomyoma, one was observed and the other was treated with a wedge resection of all the lung nodules8,9.
In conclusion, benign metastasizing leiomyoma is a rare entity that usually affects women after a hysterectomy or myomectomy for leiomyoma. The lesions are usually discovered incidentally and have an indolent clinical course. The lung is the most common site of metastatic involvement. Therefore, benign metastasizing leiomyoma should be considered for any asymptomatic patient presenting with multiple pulmonary nodules and a history of uterine leiomyoma.





 XML Download
XML Download