

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
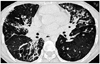
Serum CA 125 is the most useful marker for monitoring patients with epithelial ovarian cancer. However, it can be elevated above normal level in a variety of conditions other than ovarian cancer such as endometriosis, pelvic inflammation disease, and other malignant or nonmalignant disorders, including pulmonary diseases. Recently, we experienced a case of bronchiectasis in which the serum CA 125 level was elevated, changing with the patient's condition. There was no evidence of underlying malignant disease on positron emission tomography or on gynecologic examination, including transvaginal ultrasonography. During follow-up for 14 months, we could not find any clue of malignant disease that could have been the cause of the elevated levels of serum CA 125. Elevated serum CA 125 level should be interpreted carefully according to the patient's clinical condition. In addition, our case suggests that CA 125 may be used as a surrogate marker for acute inflammatory status for chronic pulmonary diseases.
Figures and Tables


References
1. Bast RC Jr, Xu FJ, Yu YH, Barnhill S, Zhang Z, Mills GB. CA 125: the past and the future. Int J Biol Markers. 1998. 13:179–187.
2. Topalak O, Saygili U, Soyturk M, Karaca N, Batur Y, Uslu T, et al. Serum, pleural effusion, and ascites CA-125 levels in ovarian cancer and nonovarian benign and malignant diseases: a comparative study. Gynecol Oncol. 2002. 85:108–113.
3. Buamah P. Benign conditions associated with raised serum CA-125 concentration. J Surg Oncol. 2000. 75:264–265.
4. Miralles C, Orea M, España P, Provencio M, Sánchez A, Cantos B, et al. Cancer antigen 125 associated with multiple benign and malignant pathologies. Ann Surg Oncol. 2003. 10:150–154.
5. Marechal F, Berthiot G, Deltour G. Serum levels of CA-50, CA-19.9, CA-125, CA-15.3, enolase and carcinoembryonic antigen in non neoplastic diseases of the lung. Anticancer Res. 1988. 8:677–680.
6. Sevinc A, Camci C, Turk HM, Buyukberber S. How to interpret serum CA 125 levels in patients with serosal involvement? A clinical dilemma. Oncology. 2003. 65:1–6.
7. Meyer T, Rustin GJ. Role of tumour markers in monitoring epithelial ovarian cancer. Br J Cancer. 2000. 82:1535–1538.
8. Bischof P. What do we know about the origin of CA 125? Eur J Obstet Gynecol Reprod Biol. 1993. 49:93–98.
9. Ozsahin SL, Turgut B, Nur N, Dogan OT, Erselcan T, Berk S. Validity of the CA125 level in the differential diagnosis of pulmonary tuberculosis. Jpn J Infect Dis. 2008. 61:68–69.
10. Kodama T, Satoh H, Ishikawa H, Ohtsuka M. Serum levels of CA19-9 in patients with nonmalignant respiratory diseases. J Clin Lab Anal. 2007. 21:103–106.
11. Yilmaz A, Ece F, Bayramgürler B, Akkaya E, Baran R. The value of CA 125 in the evaluation of tuberculosis activity. Respir Med. 2001. 95:666–669.
 XML Download
XML Download