

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
While receiving appropriate treatment, patients with tuberculosis occasionally have unusual, paradoxical reactions, with transient worsening of lesions or the development of new lesions. This report is a case of tuberculosis brain abscess and tuberculosis peritonitis with intra-abdominal abscess that developed during appropriate anti-tuberculosis chemotherapy. A 45-year-old male patient had been diagnosed as with all-drug susceptible pulmonary tuberculosis with pleurisy. Subsequently, the patient underwent standard treatment with anti-tuberculosis therapy; the pulmonary lesions improved. Three months after initial treatment, the patient developed brain abscesses and peritonitis. With the addition of corticosteroid treatment, the patient's neurologic symptoms were relieved. Exploratory laparotomy with surgical drainage was performed and a diagnosis of tuberculosis peritonitis was confirmed on biopsy. Anti-tuberculosis therapy was continued for 19 months, the patient improved eventually without further complications, although the therapeutic regimen had not been altered. In this case, the paradoxical response to treatment may have been involved in the pathogenesis of disease.
Figures and Tables
Figure 1
(A) Chest X-ray at antituberculous chemotherapy initiation. Marked left pleural effusion was found. Loculated effusion on right upper lobe also noted. (B) Chest X-ray at 3 months after antituberculous chemotherapy. Left pleural effusion completely resolved. Loculated effusion on right upper lobe also disappeared.
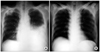
Figure 2
(A) T1 enhance axial image of brain MR on admission day. Thick ring enhanced cystic lesion on left sylvian fissure area was detected. (B) T2 enhance coronal image of brain MR on admission day. Marked periregional edema with midline shifting also detected.

Figure 3
Contrast-enhanced abdomen computed tomography at admission 11 days later. Intra abdominal fluid collection with irregular peritoneal line was noted.
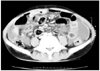
Figure 4
Contrast-enhanced brain computed tomography (CT) scanning of patient. (A) Brain CT at 9 months after treatment. Thin-walled low attenuation area on left temporoparietal lobe lesion was shown. Marked perilesional edema and midline shifting also noted. Newly developed lesion was not seen. (B) Brain CT at 13 months after treatment. Left temporoparietal abscess was mild decreased. Perilesional edema much decreased. (C) Brain CT at 17 months after treatment. Left temporoparietal abscess was considerably decreased. (D) Brain CT at 23 months after treatment. Abscess size and edema more decreased. (E) Brain CT at 32 months after treatment. Abscess size and edema much improved.

References
1. Cheng VC, Ho PL, Lee RA, Chan KS, Chan KK, Woo PC, et al. Clinical spectrum of paradoxical deterioration during antituberculosis therapy in non-HIV-infected patients. Eur J Clin Microbiol Infect Dis. 2002. 21:803–809.
2. Hung SC, Chang SC. New pulmonary lesions during therapy for extrapulmonary tuberculosis. Chest. 1999. 116:1794–1797.
3. Onal IK, Bayraktar Y, Unal S. Paradoxical deterioration during the course of antituberculous treatment. J Natl Med Assoc. 2006. 98:954–955.
4. Al-Majed SA. Study of paradoxical response to chemotherapy in tuberculous pleural effusion. Respir Med. 1996. 90:211–214.
5. Campbell IA, Dyson AJ. Lymph node tuberculosis: a comparison of various methods of treatment. Tubercle. 1977. 58:171–179.
6. Kim SH, Chung HY, Lee GD, Shin MG, Jung TS, Jin BC, et al. Clinical characteristics of paradoxical response to chemotherapy in pulmonary tuberculosis. Tuberc Respir Dis. 2002. 53:27–35.
7. Narita M, Ashkin D, Hollender ES, Pitchenik AE. Paradoxical worsening of tuberculosis following antiretroviral therapy in patients with AIDS. Am J Respir Crit Care Med. 1998. 158:157–161.
8. Ha CY, Kim JY, Kim GC, Ryeom HK, Kim HJ, Lee HJ, et al. An intraperitoneal tuberculous abscess: computed tomography (CT) findings and clinical course. Korean J Med. 2008. 74:243–249.
9. Afghani B, Lieberman JM. Paradoxical enlargement or development of intracranial tuberculomas during therapy: case report and review. Clin Infect Dis. 1994. 19:1092–1099.
10. Meintjes G, Rangaka MX, Maartens G, Rebe K, Morroni C, Pepper DJ, et al. Novel relationship between tuberculosis immune reconstitution inflammatory syndrome and antitubercular drug resistance. Clin Infect Dis. 2009. 48:667–676.
11. Marshall BG, Chambers MA. Central nervous system tuberculosis: the paradox of the host immune response. J Infect. 1998. 36:3–4.
12. Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN, et al. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med. 2003. 167:603–662.
13. Kim JY, Kwon JH, Kim MJ, Chang HW, Hwang JS, Cho KB, et al. Paradoxical response during antituberculous treatment for abdominal tuberculosis. J Korean Radiol Soc. 2006. 55:599–605.
14. de Castro CC, de Barros NG, Campos ZM, Cerri GG. CT scans of cranial tuberculosis. Radiol Clin North Am. 1995. 33:753–769.
 XML Download
XML Download