

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Churg-Strauss syndrome (CSS) or allergic granulomatous angiitis is a rare syndrome that is characterized by hypereosinophilic systemic necrotizing vasculitis affecting small- to medium-sized arteries and veins. In general, it occurs in individuals with pre-existing allergic asthma. When CSS appears in patients, it has the following characteristics: eosinophilia of more than 10% in peripheral blood, paranasal sinusitis, pulmonary infiltrates, histological proof of vasculitis with extravascular eosinophils, and mononeuritis multiplex or polyneuropathy. Therapeutic trials dedicated to Churg-Strauss syndrome have been limited due to the rarity of this disorder and the difficulty in making a histological diagnosis. Proper treatment of patients with CSS is not widely known. In this case study, we report on our experience with an unusual patient case, characterized by purpura and a perforation of the small intestine after inadequate steroid therapy.
Figures and Tables
 | Figure 1Chest radiography from 25 years old patient shows bilateral pleural effusion, patchy consolidation and increased interstitial marking of right lower lung field.
|
 | Figure 2Computed tomography from the presented patient, there are multiple, variable-sized, nodules, or nodular airspace consolidation in both lungs (A). At lower area of lung shows mild bronchial dilatation, bronchial wall thickening and tiny centrilobular branching opacities (B).
|
 | Figure 3Photography from purpura, which was stained by hematoxylin and eosin (H&E), shows epidermal hyperkeratosis and extravasated erythrocytes beneath of epidermis (arrow, A, ×40). Magnified pictures from same patient shows leukocytoclastic vasculitis with granulma formation at the perivenular area of dermal area (B, ×100), and marked neutrophils and eosinophils were infiltrated at dermal area (C, ×200).
|
 | Figure 4Colonoscopic findings from the presented patient who had abdominal pain and diarrhea, shows multiple ulceration and mucosal edema. Findings of biopsy are eosinophilic infiltration and edema at the small and medium sized vessels.
|
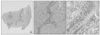 | Figure 5Specimen from resected small intestine were combined with ulcerated area, perivascular infiltration of inflammatory cells and fibrin thrombus and fibronoid necrosis (A, H&E stain, ×40; B, H&E stain, ×100). Magnified finding of perivascular area showed marked infiltration of eosinophils and neutrophils which were compatible with eosinophilic leukocytoclastic vasculitis (C, H&E stain, ×200). Some other area showed granulation tissue with hemorrhage (not shown).
|
References
1. Churg J, Strauss L. Allergic granulomatosis, allergic angiitis, and periarteritis nodosa. Am J Pathol. 1951. 27:277–301.
2. Keogh KA, Specks U. Churg-Strauss syndrome: update on clinical, laboratory and therapeutic aspects. Sarcoidosis Vasc Diffuse Lung Dis. 2006. 23:3–12.
3. Kurita M, Niwa Y, Hamada E, Hata Y, Oshima M, Mutoh H, et al. Churg-Strauss syndrome (allergic granulomatous angiitis) with multiple perforating ulcers of the small intestine, multiple ulcers of the colon, and mononeuritis multiplex. J Gastroenterol. 1994. 29:208–213.
4. Jung SH, Kim KH, Nam SM, Park HC, Chu HK, Whang IS, et al. A case of Churg-Strauss syndrome with manifestations of esophageal ulcer, acute acalculous cholecystitis and ischemic colitis. Korean J Med. 1993. 45:369–375.
5. Kim JH, Yoon KY, Shin YM. Churg-Strauss syndrome with multiple small bowel perforation. J Korean Surg Soc. 1998. 54:148–152.
6. Kim YB, Choi SW, Park IS, Han JY, Hur YS, Chu YC. Churg-Strauss syndrome with perforating ulcers of the colon. J Korean Med Sci. 2000. 15:585–588.
7. Oh MJ, Ji SH, Lim DH, Min TH, Lee BJ, Choi DC, et al. A case of intestinal perforation in Churg-Strauss syndrome patient. Korean J Med. 2004. 67:208–212.
8. Lee YK, Choi KW, Lee CY, Kim Hs, Kim KH, Kim YH. A case of Churg-Strauss syndrome associated with small bowel perforation following high dose systemic steroid intravenous injection. Korean J Dermatol. 2008. 46:950–954.
9. Vaglio A, Martorana D, Maggiore U, Grasselli C, Zanetti A, Pesci A, et al. HLA-DRB4 as a genetic risk factor for Churg-Strauss syndrome. Arthritis Rheum. 2007. 56:3159–3166.
10. Lanham JG, Elkon KB, Pusey CD, Hughes GR. Systemic vasculitis with asthma and eosinophilia: a clinical approach to the Churg-Strauss syndrome. Medicine (Baltimore). 1984. 63:65–81.
11. Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA, Arend WP, et al. The American college of rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990. 33:1094–1100.
12. Guillevin L, Cohen P, Gayraud M, Lhote F, Jarrousse B, Casassus P. Churg-Strauss syndrome: clinical study and long-term follow-up of 96 patients. Medicine (Baltimore). 1999. 78:26–37.
13. Chumbley LC, Harrison EG Jr, DeRemee RA. Allergic granulomatosis and angiitis (Churg-Strauss syndrome): report and analysis of 30 cases. Mayo Clin Proc. 1977. 52:477–484.
14. Kaneki T, Kawashima A, Hayano T, Honda T, Kubo K, Koizumi T, et al. Churg-Strauss syndrome (allergic granulomatous angitis) presenting with ileus caused by ischemic ileal ulcer. J Gastroenterol. 1998. 33:112–116.
15. Guillevin L, Lhote F, Gayraud M, Cohen P, Jarrousse B, Lortholary O, et al. Prognostic factors in polyarteritis nodosa and Churg-Strauss syndrome: a prospective study in 342 patients. Medicine (Baltimore). 1996. 75:17–28.
 XML Download
XML Download