

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
There are several respiratory diseases that show chronic granulomatous inflammation for the histologic finding. Among them, sarcoidosis and tuberculosis are not easy to differentiate when the clinical and radiological features present similar patterns. The increasing incidence of nontuberculous mycobacteria pulmonary disease is making it more difficult for clinicians to arrive at a proper diagnosis. A 69 year old male patient visited our hospital with chronic cough as his chief compliant. His radiologic findings were multiple enlarged mediastinal lymphadenpathies with innumerable micronodules and multiple patch infiltrations. The spleen biopsy finding showed chronic granulomatous inflammation, and Mycobacterium avium was identified on the bronchoscopic culture. Because of these findings, we treated him with drugs for nontuberculous mycobacteria disease other than sarcoidosis. However, during the treatment, his symptoms and radiological features became aggravated. Thus, we reviewed the radiologic and pathologic findings and decided to treat him with steroid, which relieved his symptoms and improved the radiologic findings. We report here on a case of sarcoidosis that was initially misdiagnosed as nontuberculous mycobacteria pulmonary disease.
Figures and Tables
Figure 1
His initial chest X-ray showed multiple ill-defined nodular opacities with patch consolidations in both lung fields.

Figure 2
His initial chest CT scan showed several enlarged mediastinal lymph nodes with innumerable discrete micronodules with some patch infiltrations in both lung fields. Multiple small hypodense nodules were also seen in the enlarged spleen.
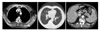
Figure 3
A spleen biopsy reveals diffuse granulomatous inflammation with some multinucleated giant cells in the fibrotic background (H&E stain, A: ×100, B: ×200).

Figure 4
(A) Before steroid treatment, previously noted multiple enlarged mediastinal lymph nodes with innumerable discrete micronodules with some patch infiltrations were increased. Splenic lesions were also increased in size and number, resulting in advanced splenomegaly. (B) After steroid treatment, multiple enlarged nodes with lung infiltrations were decreased in size and number. Also splenic lesions were significantly decreased in size and number.

References
1. Inoue Y, Suga M. Granulomatous diseases and pathogenic microorganism. Kekkaku. 2008. 83:115–130.
2. The Korean Society of Pathologist. Textbook of pathology. 2007. 6th ed. Seoul: Komoonsa.
3. Scientific committee in Korean academy of tuberculosis and respiratory diseases. National survey of sarcoidosis in Korea. Tuberc Respir Dis. 1992. 39:453–473.
4. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007. 357:2153–2165.
5. Kim DS, Ahn JJ. Sarcoidosis in Korea. Tuberc Respir Dis. 2000. 49:274–280.
6. Koyama T, Ueda H, Togashi K, Umeoka S, Kataoka M, Nagai S. Radiologic manifestations of sarcoidosis in various organs. Radiographics. 2004. 24:87–104.
7. Datta SN, Freeman A, Amerasinghe CN, Rosenbaum TP. A case of scrotal sarcoidosis that mimicked tuberculosis. Nat Clin Pract Urol. 2007. 4:227–230.
8. You IC, Moon HJ, Mun GH, Im SC, Yoon KC. A case of sarcoidosis presented as multiple conjunctival and nasal mucosal nodule. J Korean Ophthalmol Soc. 2008. 49:1000–1006.
9. Lee DY, Kim DH, Yu SY, Kwak HW. A case of sarcoidosis misdiagnosed as tuberculosis in the early phase. J Korean Ophthalmol Soc. 2004. 45:438–443.
 XML Download
XML Download