

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
The quality of care for patients with community acquired pneumonia needs to be improved; the factors affecting this care need to be analyzed. The objectives of this study were used to measure the performance of care processes of for patients with pneumonia and to determine those patient and hospital characteristics are associated with quality care.
Methods
The analysis was performed using data from 21 hospitals that had over 500 beds for 1,001 patients, who were sampled randomly. All patients were born before 31 December 1989, and discharged between the two months' August 2006 and October 2006. Performance process indicators were measured by respective hospital, and multivariate logistic regression was used to calculate associations between patients and hospital characteristics using 4 process indicators.
Results
Performance rates in timely assessment of oxygenation assessments and blood cultures, correct administration of antibiotic medications, and blood culture performed prior to initial antibiotics were 69.4%, 79.1%, 82.5% and 60.5%, respectively. Age had a positive affect on oxygenation assessment within 24 hours. Bed number, number of nurses per bed, annual number of emergency department visits, average percentage of beds filled, location and arrival time, and site were factors associated with process indicators.
Conclusion
It is necessary to make up for the weak points in the process of care for patients with community acquired pneumonia, by enforcing quality assurance. To reduce performance rate variation among hospitals, improvement in care protocols is required for hospitals that have poor quality of care levels.
Figures and Tables
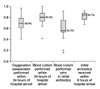 | Figure 1Medians and variation of process indicators among hospitals. Data are presented as box-and-whisker plot. The horizontal line represents the median, and upper and lower margins illustrate first and third quartile each. Upper and lower end of the vertical line means maximun and minimum value except outliers which are marked with bullet.
|




References
1. Annual report on the cause of death statistics. Korea National Statistical Office. 2008. Daejeon: Korea National Statistical Office;Available from: http://www.kosis.kr.
2. National Health Insurance Corporation, Health Insurance Review & Assessment Service. National health insurance statistical yearbook, 2006. 2007. Seoul: National Health Insurance Corporation, Health Insurance Review & Assessment Service.
3. Colice GL, Morley MA, Asche C, Birnbaum HG. Treatment costs of community-acquired pneumonia in an employed population. Chest. 2004. 125:2140–2145.
4. Meehan TP, Fine MJ, Krumholz HM, Scinto JD, Galusha DH, Mockalis JT, et al. Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA. 1997. 278:2080–2084.
5. Bratzler DW, Nsa W, Houck PM. Performance measures for pneumonia: are they valuable, and are process measure adequate? Curr Opin Infect Dis. 2007. 20:182–189.
6. Fine JM, Fine MJ, Galusha D, Petrillo M, Meehan TP. Patient and hospital characteristics associated with recommended processes of care for elderly patients hospitalized with pneumonia: results from the medicare quality indicator system pneumonia module. Arch Intern Med. 2002. 162:827–833.
7. Mitchiner JC, Hutto SL. The effect of selected hospital characteristics on the timeliness of antibiotic administration for pneumonia. Am J Med Qual. 2007. 22:259–264.
8. Dedier J, Singer DE, Chang Y, Moore M, Atlas SJ. Process of care, illness severity, and outcomes in the management of community-acquired pneumonia at academic hospitals. Arch Intern Med. 2001. 161:2099–2104.
9. Ministry for Health and Welfare. Seoul National University College of Medicine. Analyzing the results of model interpretation of clinical quality indicator. 2007. Seoul: Ministry for Health and Welfare.
10. Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997. 336:243–250.
11. Meehan TP, Weingarten SR, Holmboe ES, Mathur D, Wang Y, Petrillo MK, et al. A statewide initiative to improve the care of hospitalized pneumonia patients: The Connecticut Pneumonia Pathway Project. Am J Med. 2001. 111:203–210.
12. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007. 44:Suppl 2. S27–S72.
13. [Guidelines on the management of community-acquired pneumonia in adults]. The Korean Academy of Tuberculosis and Respiratory Diseases. 2007. Seoul: The Korean Academy of Tuberculosis and Respiratory Diseases;Available from: http://www.lungkorea.com/thesis/guide.php.
14. Houck PM, Bratzler DW, Nsa W, Ma A, Bartlett JG. Timing of antibiotic administration and outcomes for Medicare patients hospitalized with community-acquired pneumonia. Arch Intern Med. 2004. 164:637–644.
 XML Download
XML Download