

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
There are various etiologies causing bronchiectasis, but the cases without definite causes account for a quite high proportion. It is also uncertain that immunoglobulin G subclass deficiency (IgGSD) is associated with bronchiectasis. Therefore, we tried to measure the frequency of IgGSD in patients with bronchiectasis of unclear etiology, and to observe the clinical features of those patients with bronchiectasis and IgGSD.
Methods
For the outpatients of a university hospital who were diagnosed as bronchiectasis by chest CT, we produced comprehensive history taking and physical examinations, and finally selected 31 patients with bronchiectasis of unclear etiology.
Results
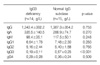
Two patients had total immunoglobulin G deficiency. The frequency of IgGSD was comparatively high (n=14). When we compared IgGSD group to normal immunoglobulin G subclass group, there were no significant differences in sex, age, and the frequency of sinusitis, bronchial asthma, and the abnormal lung function.
Figures and Tables


References
1. Barker AF. Bronchiectasis. N Engl J Med. 2002. 346:1383–1393.
2. Weycker D, Edelsberg J, Oster G, Tino G. Prevalence and economic burden of bronchiectasis. Clin Pulm Med. 2005. 12:205–209.
3. De Gracia J, Rodrigo MJ, Morell F, Vendrell M, Miravitlles M, Cruz MJ, et al. IgG subclass deficiencies associated with bronchiectasis. Am J Respir Crit Care Med. 1996. 153:650–655.
4. De Gracia J, Vendrell M, Alvarez A, Pallisa E, Rodrigo MJ, De la Rosa D, et al. Immunoglobulin therapy to control lung damage in patients with common variable immunodeficiency. Int Immunopharmacol. 2004. 4:745–753.
5. King PT, Hutchinson P, Holmes PW, Freezer NJ, Bennett-Wood V, Robins-Browne R, et al. Assessing immune function in adult bronchiectasis. Clin Exp Immunol. 2006. 144:440–446.
6. Stead A, Douglas JG, Broadfoot CJ, Kaminski ER, Herriot R. Humoral immunity and bronchiectasis. Clin Exp Immunol. 2002. 130:325–330.
7. Hill SL, Mitchell JL, Burnett D, Stockley RA. IgG subclasses in the serum and sputum from patients with bronchiectasis. Thorax. 1998. 53:463–468.
8. Bonilla FA, Bernstein IL, Khan DA, Ballas ZK, Chinen J, Frank MM, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. Ann Allergy Asthma Immunol. 2005. 94:S1–S63.
9. Maguire GA, Kumararatne DS, Joyce HJ. Are there any clinical indications for measuring IgG subclasses? Ann Clin Biochem. 2002. 39:374–377.
10. Meyts I, Bossuyt X, Proesmans M, De B. Isolated IgG3 deficiency in children: to treat or not to treat? Case presentation and review of the literature. Pediatr Allergy Immunol. 2006. 17:544–550.
11. Armenaka M, Grizzanti J, Rosenstreich DL. Serum immunoglobulins and IgG subclass levels in adults with chronic sinusitis: evidence for decreased IgG3 levels. Ann Allergy. 1994. 72:507–514.
 XML Download
XML Download