

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Idiopathic bronchiolocentric interstitial pneumonia is one of idiopathic interstitial pneumonia, which has a relatively aggressive course and poor prognosis. It is characterized by diffuse centrilobular nodules radiologically with mainly bronchiolocentric inflammation and fibrosis associated with patchy alveolitis lacking interstitial granuloma histologically. This disorder is a recently classified disease category, and to our knowledge, there is no case report in Korea. We present a case of idiopathic bronchiolocentric interstitial pneumonia. A 62-year-old man presented with exertional dyspnea with a 1 month duration. The radiological findings showed extensive centrilobular lesions at both lungs. The surgical lung biopsy specimen demonstrated a centrilobular inflammatory process with small airway fibrosis and inflammation partially radiating into the interstitium. Therefore, the patient was diagnosed with idiopathic bronchiolocentric interstitial pneumonia. He was treated with immunosuppressants including steroids and azathioprine. However, his symptoms did not improve and he expired 7 months later due to an acute exacerbation of the interstitial pneumonia and probable infectious pneumonia.
Figures and Tables

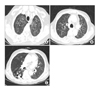
Figure 2
Chest CT demonstrates innumerable tiny centrilobular nodules in whole lung fields (A, B). There are irregular linear densities or reticulations in both lower lobes, suggesting fibrosis (C).
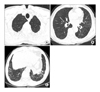
Figure 3
Biopsy of the left lung shows centrilobular inflammatory cell infiltrations and fibrosis with extension to bronchovascular bundLe and perivascular zone of the distal pulmonary lobule, which distorts brochioloalveolar strutures with relative sparing subpleural area at low magnification (A, H&E stain, ×100). High power field image shows that the lymphocytic infiltrates occasionally involve alveolar wall and that foamy macrophages aggregation with fibroblastic plug formation is found in alveolar spaces (B, H&E stain, ×200).

References
1. American Thoracic Society. European Respiratory Society. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus. Classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2002. 165:277–304.
2. Yousem SA, Dacic S. Idiopathic bronchiolocentric interstitial pneumonia. Mod Pathol. 2002. 15:1148–1153.
3. Churg A, Myers J, Suarez T, Gaxiola M, Estrada A, Mejia M, et al. Airway-centered interstitial fibrosis: a distinct form of aggressive diffuse lung disease. Am J Surg Pathol. 2004. 28:62–68.
4. Coleman A, Colby TV. Histologic diagnosis of extrinsic allergic alveolitis. Am J Surg Pathol. 1988. 12:514–518.
5. de Carvalho ME, Kairalla RA, Capelozzi VL, Deheinzelin D, do Nascimento Saldiva PH, de Carvalho CR. Centrilobular fibrosis: a novel histological pattern of idiopathic interstitial pneumonia. Pathol Res Pract. 2002. 198:577–583.
6. Mark EJ, Ruangchira-urai R. Bronchiolitis interstitial pneumonitis: a pathologic study of 31 lung biopsies with features intermediate between bronchiolitis obliterans organizing pneumonia and usual interstitial pneumonitis, with clinical correlation. Ann Diagn Pathol. 2008. 12:171–180.
 XML Download
XML Download