

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Churg-Strauss syndrome (CSS) is a disorder that is characterized by asthma, hypereosinophilia and systemic vasculitis affecting a number of organs. The manifestations of acute cholecystitis and diffuse alveolar hemorrhage are rarely reported in CSS. A 22-year-old woman with bronchial asthma visited our hospital complaining of right upper quadrant pain with a sudden onset. The abdominal computed tomography (CT) scan revealed gall bladder edema consistent with acute cholecystitis. On the initial evaluation, marked hypereosinophilia was observed in the peripheral blood smear. The nerve conduction velocity measurements and a skin biopsy performed to confirm the organ involvement of disease indicated typical mononeuritis multiplex and necrotizing vasculitis, respectively, which was complicated with CSS. On the 12th hospital day, ground glass opacity and consolidations were newly developed on both lung fields. The bronchoalveolar lavage (BAL) fluid showed increasing bloody return in sequential aliquots that were characteristic of a diffuse alveolar hemorrhage. We report a case of CSS with acute cholecystitis and diffuse alveolar hemorrhage.
Figures and Tables

Figure 2
Abdomen CT scan shows gall bladder wall thickening without stone which suggests achalculous cholecystitis.
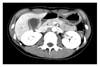
Figure 3
Microscopic findings of skin biopsy. (A) Infiltration of inflammatory cells were seen from the dermis to subcutaneous fat tissue (H&E stain, ×40). (B) Vascular wall was destroyed and showed fibrinoid change which means vasculitis. Numerous infiltrated eosinophils were also seen (H&E stain, ×400).

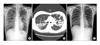
Figure 4
(A) Chest X-ray at hospital day 12 shows ground glass opacities and patchy consolidation in both lung field. (B) Chest CT scan shows lobular consolidation and ground glass opacities on both lung. Some centrilobular nodules were also seen. Lobular consolidation was mainly located at peripheral portion of both lungs. (C) Chest X-ray after treatment with methylprednisolone.
References
1. Churg J, Strauss L. Allergic granulomatosis, allergic angiitis and periarteritis nodosa. Am J Pathol. 1951. 27:277–301.
2. Kurita M, Niwa Y, Hamada E, Hata Y, Oshima M, Mutoh H, et al. Churg-Strauss syndrome (allergic granulomatous angiitis) with multiple perforating ulcers of the small intestine, multiple ulcers of the colon, and mononeuritis multiplex. J Gastroenterol. 1994. 29:208–213.
3. Suzuki M, Nabeshima K, Miyazaki M, Yoshimura H, Tagawa S, Shiraki K. Churg-Strauss syndrome complicated by colon erosion, acalculous cholecystitis and liver abscesses. World J Gastroenterol. 2005. 11:5248–5250.
4. Nishie M, Tomiyama M, Kamijo M, Kannari K, Tanosaki M, Baba M, et al. Acute cholecystitis and duodenitis associated with Churg-Strauss syndrome. Hepatogastroenterology. 2003. 50:998–1002.
5. Rolla G, Tartaglia N, Motta M, Ferrero N, Bergia R, Guida G, et al. Warning nonrespiratory symptoms in asthma: catastrophic abdominal involvement in a case of Churg-Strauss syndrome. Ann Allergy Asthma Immunol. 2007. 98:595–597.
6. Tatsukawa H, Nagano S, Umeno Y, Oribe M. Churgstrauss syndrome with cholecystitis and renal involvement. Intern Med. 2003. 42:893–896.
7. Jung SH, Kim KH, Nam SM, Park HC, Chu HK, Whang IS, et al. A case of Churg-Strauss syndrome with manifestations of esophageal ulcer, acute acalculous cholecystitis and ischemic colitis. Korean J Med. 1993. 45:369–375.
8. Kim MS, Cho YJ, Roh SH. A case of Churg-Strauss syndrome which first presented as acute cholecystitis. J Asthma Allergy Clin Immunol. 2008. 28:143–147.
9. Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA, Arend WP, et al. The American college of rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990. 33:1094–1100.
10. Clutterbuck EJ, Pusey CD. Severe alveolar haemorrhage in Churg-Strauss syndrome. Eur J Respir Dis. 1987. 71:158–163.
11. Lai RS, Lin SL, Lai NS, Lee PC. Churg-Strauss syndrome presenting with pulmonary capillaritis and diffuse alveolar hemorrhage. Scand J Rheumatol. 1998. 27:230–232.
12. Schnabel A, Reuter M, Csernok E, Richter C, Gross WL. Subclinical alveolar bleeding in pulmonary vasculitides: correlation with indices of disease activity. Eur Respir J. 1999. 14:118–124.
13. Yoshihara K, Arimura Y, Kobayashi O, Minoshima S, Kobayashi M, Yomogita S, et al. Clinical study on five myeloperoxidase specific anti-neutrophil cytoplasmic antibody (MPO-ANCA) positive Churg-Strauss syndrome cases. Ryumachi. 1998. 38:696–704.
14. Franssen C, Gans R, Kallenberg C, Hageluken C, Hoorntje S. Disease spectrum of patients with antineutrophil cytoplasmic autoantibodies of defined specificity: distinct differences between patients with anti-proteinase 3 and anti-myeloperoxidase autoantibodies. J Intern Med. 1998. 244:209–216.
15. Guillevin L, Lhote F, Gayraud M, Cohen P, Jarrousse B, Lortholary O, et al. Prognostic factors in polyarteritis nodosa and Churg-Strauss syndrome. A prospective study in 342 patients. Medicine (Baltimore). 1996. 75:17–28.
 XML Download
XML Download