

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Yun Su Sim, M.D.1, Jin Hwa Lee, M.D.1, 2 , Yon Ju Ryu, M.D.1, Eun Mi Chun, M.D.1, Jung Hyun Chang, M.D.1
, Yon Ju Ryu, M.D.1, Eun Mi Chun, M.D.1, Jung Hyun Chang, M.D.1
, Yon Ju Ryu, M.D.1, Eun Mi Chun, M.D.1, Jung Hyun Chang, M.D.1
Abstract
Background
Osteoporosis is a significant comorbidity in patients with chronic obstructive pulmonary disease (COPD). This study examined the prevalence and risk factors associated with osteoporosis in patients with COPD.
Methods
The bone mineral densities (BMDs) of the lumbar spine and femoral bone were measured in 53 patients with clinically stable COPD and 41 age- and gender-matched control subjects showing a normal lung function. Osteoporosis was defined as a T-score ≤-2.5. The subjects' clinical characteristics and laboratory data were reviewed, and multiple logistic regression analysis was used to identify the risk factors associated with osteoporosis in COPD patients.
Results
The prevalence of osteoporosis was 47% and 32% in the COPD patients and controls, respectively. In particular, using the femoral neck T-score, the prevalence of osteoporosis in COPD patients was higher than that in the controls (26% vs. 5%; p=0.006). The average T-score of the lumbar spine (p=0.025) and femoral neck of COPD patients were significantly lower than those of the controls (p=0.001). The forced expiratory volume in the 1 second (FEV1) % predicted (p=0.019; odds ratio [OR], 0.955; 95% confidence interval [CI], 0.919-0.993) and age (p=0.024; OR, 1.144; 95% CI, 1.018-1.287) were independently associated with osteoporosis in patients with COPD.
Figures and Tables


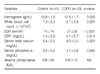
Table 4
Comparison of bone density parameters and prevalence of osteoporosis in patients with COPD and age- and sex-matched controls



References
1. Chatila WM, Thomashow BM, Minai OA, Criner GJ, Make BJ. Comorbidities in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008. 5:549–555.
2. Incalzi RA, Caradonna P, Ranieri P, Basso S, Fuso L, Pagano F, et al. Correlates of osteoporosis in chronic obstructive pulmonary disease. Respir Med. 2000. 94:1079–1084.
3. Iqbal F, Michaelson J, Thaler L, Rubin J, Roman J, Nanes MS. Declining bone mass in men with chronic pulmonary disease: contribution of glucocorticoid treatment, body mass index, and gonadal function. Chest. 1999. 116:1616–1624.
4. Shane E, Silverberg SJ, Donovan D, Papadopoulos A, Staron RB, Addesso V, et al. Osteoporosis in lung transplantation candidates with end-stage pulmonary disease. Am J Med. 1996. 101:262–269.
5. Block JE, Stubbs H. Hip fracture-associated mortality reconsidered. Calcif Tissue Int. 1997. 61:84.
6. Biskobing DM. COPD and osteoporosis. Chest. 2002. 121:609–620.
7. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001. 163:1256–1276.
8. American Thoracic Society. Standardization of Spirometry, 1994 Update. Am J Respir Crit Care Med. 1995. 152:1107–1136.
9. Kanis JA, Melton LJ 3rd, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res. 1994. 9:1137–1141.
10. Jørgensen NR, Schwarz P, Holme I, Henriksen BM, Petersen LJ, Backer V. The prevalence of osteoporosis in patients with chronic obstructive pulmonary disease: a cross sectional study. Respir Med. 2007. 101:177–185.
11. Slemenda CW, Hui SL, Longcope C, Johnston CC Jr. Cigarette smoking, obesity, and bone mass. J Bone Miner Res. 1989. 4:737–741.
12. Daniell HW. Osteoporosis and smoking. JAMA. 1972. 221:509.
13. Bassett CA, Becker RO. Generation of electric potentials by bone in response to mechanical stress. Science. 1962. 137:1063–1064.
14. Cauley JA, Salamone LM, Lucas FL. Marcus R, Feldman D, Kelsey J, editors. Postmenopausal endogenous and exogenous hormones, degree of obesity, thiazide diuretics, and risk of osteoporosis. Osteoporosis. 1996. 1st ed. New York: Academic Press;551–576.
15. Adachi JD. Corticosteroid-induced osteoporosis. Am J Med Sci. 1997. 313:41–49.
16. Lane NE, Lukert B. The science and therapy of glucocorticoid-induced bone loss. Endocrinol Metab Clin North Am. 1998. 27:465–483.
17. Canalis E. Mechanisms of glucocorticoid action in bone: implications to glucocorticoid-induced osteoporosis. J Clin Endocrinol Metab. 1996. 81:3441–3447.
18. Sevenoaks MJ, Stockley RA. Chronic Obstructive Pulmonary Disease, inflammation and co-morbidity--a common inflammatory phenotype? Respir Res. 2006. 7:70.
19. Dalsky GP, Stocke KS, Ehsani AA, Slatopolsky E, Lee WC, Birge SJ Jr. Weight-bearing exercise training and lumbar bone mineral content in postmenopausal women. Ann Intern Med. 1988. 108:824–828.
20. White MK, Martin RB, Yeater RA, Butcher RL, Radin EL. The effects of exercise on the bones of postmenopausal women. Int Orthop. 1984. 7:209–214.
21. Choi JS, An KC, Lee CS, Choi JM, Kim JY, Shin DR. DEXA T-score concordance and discordance between hip and lumbar spine. J Korean Soc Spine Surg. 2003. 10:75–81.
 XML Download
XML Download