

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Churg-Strauss syndrome is a rare form of systemic necrotizing vasculitis that occurs exclusively in patients with asthma, and is associated with blood and tissue eosinophilia. The classic pathology findings in the lung include a combination of eosinophilic pneumonia, granulomatous inflammation and necrotizing vasculitis. However, there are few reports of tracheobronchial mucosal lesions in Churg-Strauss syndrome. We report a case of Churg-Strauss syndrome with multiple tracheobronchial mucosal lesions in a 33-year-old man with a history of bronchial asthma and allergic rhinitis. He had been diagnosed with community acquired pneumonia at another hospital and was treated with antibiotics. However, the chest radiographic findings were aggravated and showed multifocal consolidations in the whole lung fields. He was transferred to the Asan Medical Center. Fiberoptic bronchoscopy revealed multiple nodular mucosal lesions of the trachea and bronchi. The histopathology of the mucosal lesions revealed necrotizing bronchial inflammation with eosinophilic infiltration. Video Assisted Thoracic Surgery was performed. The wedge resected lung tissue revealed chronic eosinophilic pneumonia that was consistent with Churg-Strauss syndrome. Methylprednisolone (1 mg/kg q 8 hr) was prescribed and his symptoms resolved gradually. The chest radiographic findings improved significantly, and a follow-up fiberoptic bronchoscopy performed eight days later showed that the tracheobronchial mucosal lesions had resolved. The patient was prescribed oral prednisolone for 20 months after discharge. Currently, the patient is not taking steroids and is being followed up.
Figures and Tables
Figure 1
(A) The chest radiography shows multifocal patchy consolidations and ground glass opacities. (B) The chest computed tomography (CT) scan shows peripherally distributed ground-glass opacities and consolidations in both lungs. (C) The chest radiography reveals improvement of the lesions, 45 days after steroid therapy.

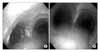
Figure 2
(A) Fiberoptic bronchoscopy shows multiple nodular mucosal lesions in the trachea and bronchi. (B) Fiberoptic bronchoscopy shows the disappearance of tracheobronchial lesions eight days after steroid therapy.

References
1. Churg J, Strauss L. Allergic granulomatosis, allergic angiitis, and periarteritis nodosa. Am J Pathol. 1951. 27:277–301.
2. Yang KJ, Moon HS, Lee WK, Song JS, Ro JC, Park SH, et al. A case of allergic granulomatosis. Tuberc Respir Dis. 1986. 33:247–251.
3. Alvarez-Sala R, Prados C, Armada E, Del Arco A, Villamor J. Congestive cardiomyopathy and endobronchial granulomas as manifestations of Churg-Strauss syndrome. Postgrad Med J. 1995. 71:365–366.
4. Matsushima H, Takayanagi N, Kurashima K, Tokunaga D, Ubukata M, Kawabata Y, et al. Multiple tracheobronchial mucosal lesions in two cases of Churg-Strauss syndrome. Respirology. 2006. 11:109–112.
5. Noth I, Strek ME, Leff AR. Churg-Strauss syndrome. Lancet. 2003. 361:587–594.
6. Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA, Arend WP, et al. The American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990. 33:1094–1100.
7. Nouraei SA, Obholzer R, Ind PW, Salama AD, Pusey CD, Porter F, et al. Results of endoscopic surgery and intralesional steroid therapy for airway compromise due to tracheobronchial Wegener's granulomatosis. Thorax. 2008. 63:49–52.
8. Daum TE, Specks U, Colby TV, Edell ES, Brutinel MW, Prakash UB, et al. Tracheobronchial involvement in Wegener's granulomatosis. Am J Respir Crit Care Med. 1995. 151:522–526.
9. Cordier JF, Valeyre D, Guillevin L, Loire R, Brechot JM. Pulmonary Wegener's granulomatosis: a clinical and imaging study of 77 cases. Chest. 1990. 97:906–912.
10. An JY, Lee JE, Park HW, Lee JH, Yang SA, Jung SS, et al. Clinical and bronchoscopic features in endobronchial tuberculosis. Tuberc Respir Dis. 2006. 60:532–539.
11. Judson MA, Sahn SA. Endobronchial lesions in HIV-infected individuals. Chest. 1994. 105:1314–1323.
12. Guillevin L, Cohen P, Gayraud M, Lhote F, Jarrousse B, Casassus P. Churg-Strauss syndrome: clinical study and long-term follow-up of 96 patients. Medicine (Baltimore). 1999. 78:26–37.
13. Solans R, Bosch JA, Perez-Bocanegra C, Selva A, Huguet P, Alijotas J, et al. Churg-Strauss syndrome: outcome and long-term follow-up of 32 patients. Rheumatology (Oxford). 2001. 40:763–771.
14. Lanham JG, Elkon KB, Pusey CD, Hughes GR. Systemic vasculitis with asthma and eosinophilia: a clinical approach to the Churg-Strauss syndrome. Medicine (Baltimore). 1984. 63:65–81.
 XML Download
XML Download