

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
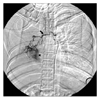
Pregnancy induces many physiologic changes, and it can cause hemoptysis in relation to the underlying or potential pulmonary diseases. Although hemoptysis is not a frequent event during pregnancy, a thorough search for its etiology and then immediate management should be initiated for a case of massive hemoptysis to avoid serious adverse effects on both the fetus and the mother. Most hemoptysis events during pregnancy are related to well known etiologies, but there are a few reported cases of hemoptysis in pregnant women who are without any underlying lung lesion. We report here on a case of a pregnant woman with total lung collapse due to hemoptysis, and a thorough search for the etiology after delivery could not reveal any etiology.
Figures and Tables


References
1. Shaikh S, Saad RA, Christie G, Kerr KM, Remmen H. Spontaneous dissection of an anomalous systemic artery in the lung during pregnancy: a rare cause of hemoptysis. Ann Thorac Surg. 2006. 82:725–726.
2. Dayoan ES, Dimen LL, Boylen CT. Successful treatment of Wegener's granulomatosis during pregnancy: a case report and review of the medical literature. Chest. 1998. 113:836–838.
3. Peyrat E, Chabbert V, Escamilla R, Saada J, Degano B. Idiopathic hemoptysis in pregnant women: a distinct entity? Respir Med. 2007. 101:2221–2223.
4. Jean-Baptiste E. Clinical assessment and management of massive hemoptysis. Crit Care Med. 2001. 29:1098.
5. Kali PB, Gray GE, Violari A, Chaisson RE, McIntyre JA, Martinson NA. Combining PMTCT with active case finding for tuberculosis. J Acquir Immune Defic Syndr. 2006. 42:379–381.
6. Huppertz B, Peeters LL. Vascular biology in implantation and placentation. Angiogenesis. 2005. 8:157–167.
7. Pratter MR. Chronic upper airway cough syndrome secondary to rhinosinus diseases (previously referred to as postnasal drip syndrome): ACCP evidence-based clinical practice guidelines. Chest. 2006. 129:63S–71S.
8. Krause DN, Duckles SP, Pelligrino DA. Influence of sex steroid hormones on cerebrovascular function. J Appl Physiol. 2006. 101:1252–1261.
 XML Download
XML Download