

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Non-resolving or slowly resolving pulmonary infiltrates in spite of administering adequate antimicrobial therapy are a clinical diagnostic challenge for physicians. The rate of radiographic resolution varies with the patients' age, the underlying comorbidities, the extent of radiographic involvement, the functional status and the causal pathogens. It is important to differentiate non-resolving or slowly resolving bacterial pneumonia from other uncommon infectious pneumonias or malignancies that require invasive diagnostic techniques to confirm the diagnosis. Bronchioloalveolar carcinoma can present with various clinical and radiographic features. Unfortunately, the radiographic similarity of consolidative BAC to pneumonia often leads to an incorrect diagnosis of pneumonia and possibly significant delays in obtaining appropriate diagnostic studies. We describe here a case of a mixed adenocarcinoma and bronchioloalveolar carcinoma that was initially diagnosed as pneumonia due to the consolidation pattern on the radiography and the patient's initial improvement with antibiotic treatment.
Figures and Tables
Figure 1
Initial chest CT (at admission) showed right lower lobe consolidation with pleural effusion and reactive LN enlargement.
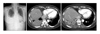
Figure 2
Chest images at 16th day after admission showed improved right lower lobe consolidation and pleural effusion after 16 days of antibiotics therapy.
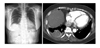
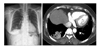
Figure 3
After 2 month of discharge, follow-up chest CT showed decreased pleural effusion but remaining consolidation was still observed at right lower lobe.

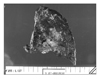
Figure 4
After 4 month of discharge, follow-up chest CT showed decreased but remaining consolidation with focal cavitation at right lower lobe.


References
1. Niederman MS. Understanding the natural history of community-acquired pneumonia resolution: vital information for optimizing duration of therapy. Clin Infect Dis. 2004. 39:1791–1793.
2. Kuru T, Lynch JP 3rd. Nonresolving or slowly resolving pneumonia. Clin Chest Med. 1999. 20:623–651.
3. El Solh AA, Aquilina AT, Gunen H, Ramadan F. Radiographic resolution of community-acquired bacterial pneumonia in the elderly. J Am Geriatr Soc. 2004. 52:224–229.
4. Thompson WH. Bronchioloalveolar carcinoma masquerading as pneumonia. Respir Care. 2004. 49:1349–1353.
5. Raz DJ, Kim JY, Jablons DM. Diagnosis and treatment of bronchioloalveolar carcinoma. Curr Opin Pulm Med. 2007. 13:290–296.
6. Read WL, Page NC, Tierney RM, Piccirillo JF, Govindan R. The epidemiology of bronchioloalveolar carcinoma over the past two decades: analysis of the SEER database. Lung Cancer. 2004. 45:137–142.
7. Sadohara J, Fujimoto K, Terasaki H, Nonoshita M, Hayabuchi N. Bronchioloalveolar carcinoma with fluctuating extent of consolidation on chest radiography. J Thorac Imaging. 2004. 19:63–66.
8. Dumont P, Gasser B, Rouge C, Massard G, Wihlm JM. Bronchoalveolar carcinoma: histopathologic study of evolution in a series of 105 surgically treated patients. Chest. 1998. 113:391–395.
9. Casey KR. Neoplastic mimics of pneumonia. Semin Respir Infect. 1995. 10:131–142.
10. Aquino SL, Chiles C, Halford P. Distinction of consolidative bronchioloalveolar carcinoma from pneumonia: do CT criteria work? AJR Am J Roentgenol. 1998. 171:359–363.
11. Kim MH, Kim CH, Kim YH, Park TW, Kang JH, Ahn MI, et al. A case of very slowly progressed pneumonic consolidation. Tuberc Respir Dis. 1996. 43:472–476.
12. Kim TH, Kim SJ, Ryu YH, Chung SY, Seo JS, Kim YJ, et al. Differential CT features of infectious pneumonia versus bronchioloalveolar carcinoma (BAC) mimicking pneumonia. Eur Radiol. 2006. 16:1763–1768.
 XML Download
XML Download