

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Angiosarcoma is a rare but highly malignant tumorthat usually arises in the scalp or face of elderly males. Distant metastases favor the lung, liver, lymph nodes and skin. Metastatic pulmonary angiosarcoma commonly takes the form of a nodule but can sometimes appear as a thin-walled cyst. We report a case of 65 years-old male with a spontaneous pneumothorax, who underwent excision and radiotherapy for an angiosarcoma of the scalp 2 years ago. A chest CT scan revealed multiple cysts in the lung. The video-assisted thoracoscopic lung biopsy demonstrated subpleural cysts without tumor cells. A skin biopsy of the scalp showed an angiosarcoma. This case was diagnosed as a recurrence of an angiosarcoma with a supposed lung metastasis. This case suggests that a spontaneous pneumothorax in elderly people may be secondary to a pulmonary metastasis from an angiosarcoma of the scalp.
Figures and Tables

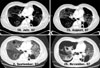
 | Figure 2When patient visited outpatient department due to repiratory symptom, Chest CT scans showed multiple cysts and ground glass opacity.
|

 | Figure 4Subpleural cyst formation was seen in viedo-assited thoracoscopic lung biopsy, but tumor cells were not seen (H&E stain, ×10).
|

References
1. Orchard GE, Zelger B, Jones EW, Jones RR. An immunocytochemical assessment of 19 cases of cutaneous angiosarcoma. Histopathology. 1996. 28:235–240.
2. Mendenhall WM, Mendenhall CM, Werning JW, Reith JD, Mendenhall NP. Cutanoues angiosarcoma. Am J Clin Oncol. 2006. 29:524–528.
3. Holden CA, Spittle MF, Jones EW. Angiosarcoma of the face and scalp, prognosis and treatment. Cancer. 1987. 59:1046–1057.
4. Mark RJ, Tran LM, Sercarz J, Fu YS, Calcaterra TC, Juillard GF. Angiosarcoma of the head and neck. The UCLA experience 1955 through 1990. Arch Otolaryngol Head Neck Surg. 1993. 119:973–978.
5. Kitagawa M, Tanaka I, Takemura T, Matsubara O, Kasuga T. Angiosarcoma of the scalp: report of two cases with fatal pulmonary complications and a review of Japanese autopsy registry data. Virchows Arch A Pathol Anat Histopathol. 1987. 412:83–87.
6. Tateishi U, Hasegawa T, Kusumoto M, Yamazaki N, Iinuma G, Muramatsu Y, et al. Metastatic angiosarcoma of the lung: spectrum of CT findings. AJR Am J Roentgenol. 2003. 180:1671–1674.
7. Sakurai H, Hada M, Miyashita Y, Tsukamoto K, Oyama T, Ashizawa I. Simultaneous bilateral spontaneous pneumothorax secondary to metastatic angiosarcoma of the scalp: report of a case. Surg Today. 2006. 36:919–922.
8. Pawlik TM, Paulino AF, McGinn CJ, Baker LH, Cohen DS, Morris JS, et al. Cutaneous angiosarcoma of the scalp: a multidisciplinary approach. Cancer. 2003. 98:1716–1726.
9. Fata F, O'Reilly E, Ilson D, Pfister D, Leffel D, Kelsen DP, et al. Paclitaxel in the treatment of patients with angiosarcoma of the scalp or face. Cancer. 1999. 86:2034–2037.
10. Budd GT. Management of angiosarcoma. Curr Oncol Rep. 2002. 4:515–519.
 XML Download
XML Download