

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Alcaligenes xylosoxidans is a catalase and oxidase positive, motile, nonfermentative and gram-negative rod bacterium. A. xylosoxidans infection is a rare cause of pulmonary infection and little information concerning treatment is available. The majority of patients that develop A. xylosoxidans infection belong to a high-risk group due to an immunocompromised condition or due to pulmonary cystic fibrosis. We report two rare cases of immunocompentent patients that developed a pulmonary infection due to A. xylosoxidans. A 77-year-old man was admitted with a lung abscess. The patient denied having any prior medical illness. A culture of bronchial washing fluid showed the presence of A. xylosoxidans. Despite appropriate antibiotic treatment, the patient died from acute respiratory distress syndrome (ARDS). Another patient, a 61-year-old man without an underlying disease, was admitted with empyema. Under the condition of a closed thoracostomy, a high fever persisted and the empyema was also aggravated. A. xylosoxidans was detected from a culture of pleural fluid. Susceptible antibiotic treatment was provided and surgical intervention was performed. We report these cases with a review of the literature.
Figures and Tables
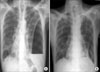
Figure 1
Case 1: Initial chest X-ray shows ill-defined mass, probably associated with peripheral collapse or pneumonic consolidation in the area of left upper lobe (A). Following chest x-ray (HOD#14), the lung abscess on the apical area of left upper lobe has decreased but pneumonic consolidation has developed at left lower lobe (B).

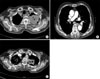
Figure 2
Case 1: Initial chest CT shows necrotic mass and cavity in the left upper lobe (A). Small amount of bilateral pleural effusion and lymphadenitis at right hilar and bilateral mediastinal areas were noted (B). Following chest CT (HOD#20) shows that the size of lung abscess has decreased at the left upper lobe (C).
References
1. Mandell WF, Garvey GJ, Neu HC. Achromobacter xylosoxidans bacteremia. Rev Infect Dis. 1987. 9:1001–1005.
2. Aisenberg G, Rolston KV, Safdar A. Bacteremia caused by Achromobacter and Alcaligenes species in 46 patients with cancer (1989-2003). Cancer. 2004. 101:2134–2140.
3. Gomez-Cerezo J, Suarez I, Rios JJ, Pena P, Garcia de Miguel MJ, de Jose M, et al. Achromobacter xylosoxidans bacteremia: a 10-year analysis of 54 cases. Eur J Clin Microbiol Infect Dis. 2003. 22:360–363.
4. Kish MA, Buggy BP, Forbes BA. Bacteremia caused by Achromobacter species in an immunocompromised host. J Clin Microbiol. 1984. 19:947–948.
5. Knippschild M, Schmid EN, Uppenkamp M, Konig E, Meusers P, Brittinger G, et al. Infection by Alcaligenes xylosoxidans subsp. xylosoxidans in neutropenic patients. Oncology. 1996. 53:258–262.
6. Legrand C, Anaissie E. Bacteremia due to Achromobacter xylosoxidans in patients with cancer. Clin Infect Dis. 1992. 14:479–484.
7. Mizunoe S, Yamasaki T, Hirai K, Yamagata E, Hiramatsu K, Yamakami Y, et al. Case report: subcutaneous abscess and thoracic empyema caused by Alcaligenes xylosoxidans. Kansenshogaku Zasshi. 1998. 72:631–634.
8. Shie SS, Huang CT, Leu HS. Characteristics of Achromobacter xylosoxidans bacteremia in northern Taiwan. J Microbiol Immunol Infect. 2005. 38:277–282.
9. Tsay RW, Lin LC, Chiou CS, Liao JC, Chen CH, Liu CE, et al. Alcaligenes xylosoxidans bacteremia: clinical features and microbiological characteristics of isolates. J Microbiol Immunol Infect. 2005. 38:194–199.
10. Weitkamp JH, Tang YW, Haas DW, Midha NK, Crowe JE Jr. Recurrent Achromobacter xylosoxidans bacteremia associated with persistent lymph node infection in a patient with hyper-immunoglobulin M syndrome. Clin Infect Dis. 2000. 31:1183–1187.
11. Igra-Siegman Y, Chmel H, Cobbs C. Clinical and laboratory characteristics of Achromobacter xylosoxidans infection. J Clin Microbiol. 1980. 11:141–145.
12. De Baets F, Schelstraete P, Van Daele S, Haerynck F, Vaneechoutte M. Achromobacter xylosoxidans in cystic fibrosis: prevalence and clinical relevance. J Cyst Fibros. 2007. 6:75–78.
13. Vay CA, Almuzara MN, Rodriguez CH, Pugliese ML, Lorenzo Barba F, Mattera JC, et al. 'In vitro' activity of different antimicrobial agents on Gram-negative nonfermentative bacilli, excluding Pseudomonas aeruginosa and Acinetobacter spp. Rev Argent Microbiol. 2005. 37:34–45.
14. Spear JB, Fuhrer J, Kirby BD. Achromobacter xylosoxidans (Alcaligenes xylosoxidans subsp. xylosoxidans) bacteremia associated with a well-water source: case report and review of the literature. J Clin Microbiol. 1988. 26:598–599.
15. Saiman L, Chen Y, Gabriel PS, Knirsch C. Synergistic activities of macrolide antibiotics against Pseudomonas aeruginosa, Burkholderia cepacia, Stenotrophomonas maltophilia, and Alcaligenes 3xylosoxidans isolated from patients with cystic fibrosis. Antimicrob Agents Chemother. 2002. 46:1105–1107.
 XML Download
XML Download