

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Benign bronchoesophageal fistula is a rare disease and it may be characterized by nonspecific symptoms that can cause a delayed diagnosis. We misdiagnosed a patient with recurrent aspiration, which was due to bronchoesophageal fistula, as active pulmonary tuberculosis. The patient was 44 year old female who had suffered from chronic cough, especially during eating liquid meals, since 1982 when she had been treated for tuberculous lymphadenitis. Computed tomography showed an irregular mass with surrounding centrilobular nodules in the superior segment of the right lower lobe (RLL). She was diagnosed as having active pulmonary tuberculosis and treated with anti-tuberculosis medication, but she continued to complain of persistent cough even after anti-tuberculosis treatment. Thus, we reexamined the patient, and bronchoesophageal fistula between the esophagus and the superior segment of the RLL was finally confirmed by esophagography. After the fistula was surgically treated, the patient became asymptomatic and she then experienced good health.
Figures and Tables
 | Figure 1Chest CT showed irregular mass with central calcification and surrounding centrilobular nodules and branching lesions in superior segment of right lower lobe.
|
 | Figure 2Chest X-ray showed multiple calcified nodules and a bulging mass with calcification at right paratracheal area.
|
 | Figure 3Chest CT showed cavitary lesion in superior segment of right lower lobe and fistulous tract (arrow) at right side of mid-esophagus.
|
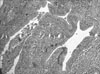
 | Figure 4Esophagography showed fistulous tract (arrow) between the esophagus and the superior segment of right lower lobe.
|
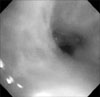 | Figure 5Bronchoscopy showed stenosis of the superior segmental bronchus of right lower lobe, but could not reveal the fistula orifice.
|
 | Figure 6Esophagogastrofiberscopy showed the fistula orifice and both fibrin glue and hemoclip were used for closing fistula orifice.
|

References
1. Lado Lado FL, Golpe Gomez A, Cabarcos Ortiz de Barron A, Antunez Lopez JR. Bronchoesophageal fistulae secondary to tuberculosis. Respiration. 2002. 69:362–365.
2. Spalding AR, Burney DP, Richie RE. Acquired benign bronchoesophageal fistulas in the adult. Ann Thorac Surg. 1979. 28:378–383.
3. Murdock A, Moorehead RJ, Tham TC. Closure of a benign bronchoesophageal fistula with endoscopic clips. Gastrointest Endosc. 2005. 62:635–638.
4. Park JH, Moon JH, Kim JH, Choi HJ, Lee JS, Hwang SC, et al. A case of tuberculous tracheoesophageal fistula. Korean J Med. 1987. 32:690–695.
5. Allen CM, Craze J, Grundy A. Tuberculous broncho-oesophageal fistula in the acquired immunodeficiency syndrome. Clin Radiol. 1991. 43:60–62.
6. Mangi AA, Gaissert HA, Wright CD, Allan JS, Wain JC, Grillo HC, et al. Benign broncho-esophageal fistula in the adult. Ann Thorac Surg. 2002. 73:911–915.
7. Cho KH, Park JH, Jeong ID, Lee BM, Kim DI, Lee JW, et al. A case of broncho-esophageal fistula treated by histoacryl (R) injection therapy. Korean J Gastrointest Endosc. 2005. 31:161–165.
8. Oh SH, Kim JK, Wie SH, Kim PS, Kang SH, Kim JI, et al. A case of tuberculous bronchoesophageal fistula. Korean J Gastrointest Endosc. 1995. 15:235–239.
9. Asnis DS, Saltzman HP, Giron JA. Bronchoesophageal fistula due to multidrug-resistant tuberculosis in a patient infected with human immunodeficiency virus. Clin Infect Dis. 1995. 21:1061–1062.
10. Dronda F, Fernandez-Martin I, Gonzalez-Lopez A, Puente L. Delayed development of tuberculous bronchoesophageal fistulas in a patient with AIDS necessitates endoscopic surgery. Clin Infect Dis. 1995. 21:1062–1063.
11. Porter JC, Friedland JS, Freedman AR. Tuberculous bronchoesophageal fistulae in patients infected with the human immunodeficiency virus: three case reports and review. Clin Infect Dis. 1994. 19:954–957.
12. Vartian CV, Septimus EJ. Bronchoesophageal fistula due to Mycobacterium tuberculosis and cytomegalovirus in a patient with AIDS. Clin Infect Dis. 1996. 22:581.
13. Alkhuja S, Miller A. Tuberculous bronchoesophageal fistulae in patients infected with the human immunodeficiency virus: a case report and review. Heart Lung. 1998. 27:143–145.
14. Chiu HH, Chen CM, Mo LR, Chao TJ. Gastrointestinal: tuberculous bronchoesophageal fistula. J Gastroenterol Hepatol. 2006. 21:1074.
15. Griffo S, Stassano P, Iannelli G, Di Tommaso L, Cicalese M, Monaco M, et al. Benign bronchoesophageal fistula: report of four cases. J Thorac Cardiovasc Surg. 2007. 133:1378–1379.
16. Gerzic Z, Rakic S, Randjelovic T. Acquired benign esophagorespiratory fistula: report of 16 consecutive cases. Ann Thorac Surg. 1990. 50:724–727.
 XML Download
XML Download